

Development and evaluation of an indirect ELISA using a multiepitope antigen for the diagnosis of intestinal schistosomiasis
- PMID: 37092694
- PMCID: PMC10410369
- DOI: 10.1017/S0031182023000409
Development and evaluation of an indirect ELISA using a multiepitope antigen for the diagnosis of intestinal schistosomiasis
Abstract
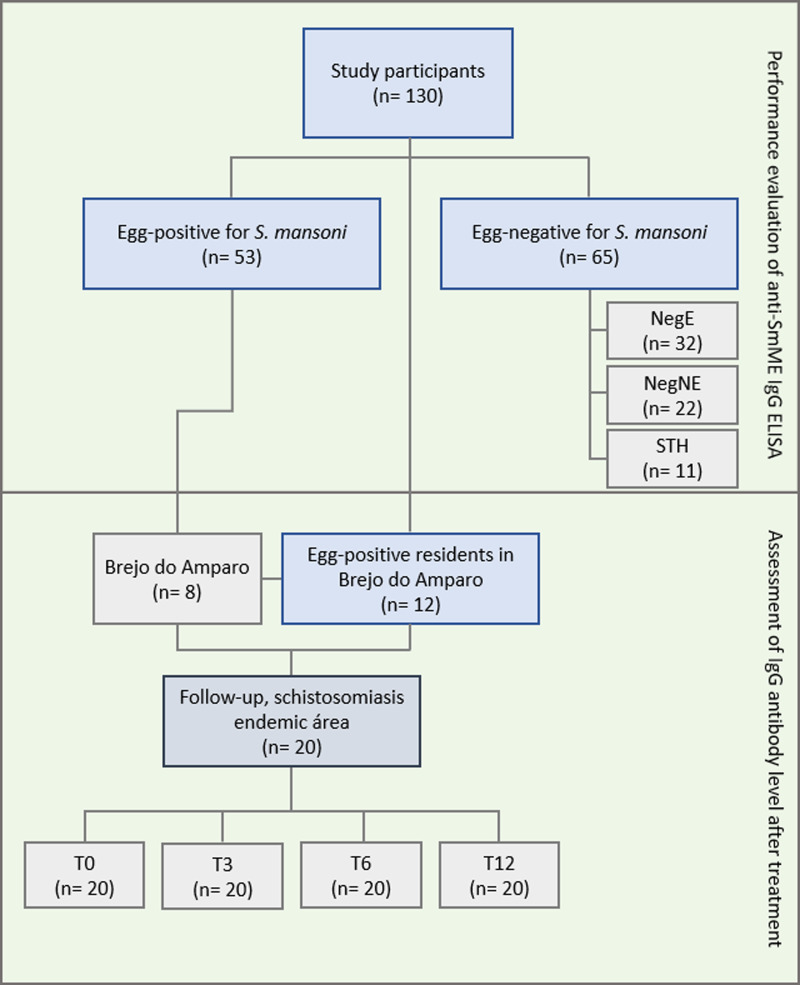
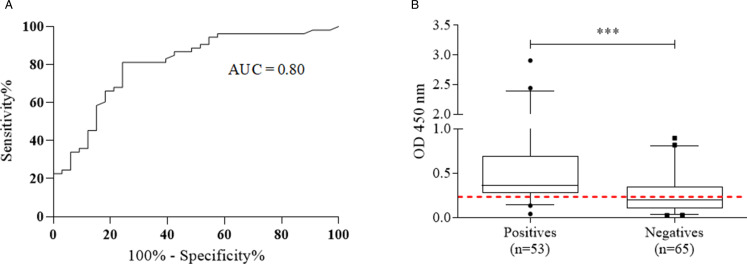
The laboratory diagnosis of intestinal schistosomiasis, carried out by detecting parasite eggs in feces, has low sensitivity when applied to individuals with low parasitic load. Serological tests can be more sensitive for the diagnosis of the disease. Therefore, the objective of this work was to develop and evaluate an ELISA-based immunoenzymatic assay, using a Schistosoma mansoni multiepitope antigen (ELISA IgG anti-SmME). For this, the amino acid sequences of S. mansoni cathepsin B and asparaginyl endopeptidase were submitted to the prediction of B cell epitopes and, together with peptide sequences obtained from earlier works, were used in the construction of a minigene. The multiepitope protein was expressed in Escherichia coli and the performance of the ELISA IgG anti-SmME for schistosomiasis was evaluated using serum samples from 107 individuals either egg positive or negative. In addition, 11 samples from individuals with other helminth infections were included. The ELISA IgG anti-SmME showed a sensitivity of 81.1% and a specificity of 46.1%. Further analysis revealed a 77.2% sensitivity in diagnosis of individuals with egg counts of ≤12 epg (eggs per gram feces) and 87.5% for individuals with 13–99 epg. It is worth mentioning that, to our knowledge, this was the first study using a multiepitope recombinant antigen in an ELISA for diagnosis of intestinal schistosomiasis, which demonstrated promising results in the diagnosis of individuals with low parasitic loads.
Keywords: Asparaginyl endopeptidase; Schistosoma mansoni; cathepsin B; diagnosis; low parasitic load; multiepitope antigen; serology.
Conflict of interest statement
The authors declare there is no conflict of interest.
Figures




Similar articles
-
Evaluation of isotype-based serology for diagnosis of Schistosoma mansoni infection in individuals living in endemic areas with low parasite burden.Acta Trop. 2023 Dec;248:107017. doi: 10.1016/j.actatropica.2023.107017. Epub 2023 Sep 28. Acta Trop. 2023. PMID: 37774894
-
Serological proteomic screening and evaluation of a recombinant egg antigen for the diagnosis of low-intensity Schistosoma mansoni infections in endemic area in Brazil.PLoS Negl Trop Dis. 2019 Mar 14;13(3):e0006974. doi: 10.1371/journal.pntd.0006974. eCollection 2019 Mar. PLoS Negl Trop Dis. 2019. PMID: 30870412 Free PMC article.
-
Rapid detection of a Schistosoma mansoni circulating antigen excreted in urine of infected individuals by using a monoclonal antibody.J Clin Microbiol. 1999 Feb;37(2):354-7. doi: 10.1128/JCM.37.2.354-357.1999. J Clin Microbiol. 1999. PMID: 9889217 Free PMC article.
-
Diagnosis of schistosomiasis mansoni: an evaluation of existing methods and research towards single worm pair detection.Parasitology. 2018 Sep;145(11):1355-1366. doi: 10.1017/S0031182018000240. Epub 2018 Mar 6. Parasitology. 2018. PMID: 29506583 Review.
-
Use of Schistosoma mansoni soluble egg antigen (SEA) for antibody detection and diagnosis of schistosomiasis: The need for improved accuracy evaluations of diagnostic tools.Acta Trop. 2021 Mar;215:105800. doi: 10.1016/j.actatropica.2020.105800. Epub 2020 Dec 23. Acta Trop. 2021. PMID: 33352167 Review.
References
-
- Baum LG and Crocker PR (2009) Glycoimmunology: ignore at your peril!. Immunological Reviews 230, 5–8. - PubMed
-
- Brasil MS (2014) Vigilância da Esquistossomose mansoni, 4th Edn. Brasília: Diretrizes Técnicas.
-
- Brindley PJ, Kalinna BH, Dalton JP, Day SR, Wong JY, Smythe ML and McManus DP (1997) Proteolytic degradation of host hemoglobin by schistosomes. Molecular and Biochemical Parasitology 89, 1–9. - PubMed
-
- Coelho PMZ, Jurberg AD, Oliveira AA and Katz N (2009) Use of a saline gradient for the diagnosis of schistosomiasis. Memórias do Instituto Oswaldo Cruz 104, 720–723. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
