

Biomarker-Based Risk Stratification in Pediatric Sepsis From a Low-Middle Income Country
- PMID: 37092821
- PMCID: PMC10317305
- DOI: 10.1097/PCC.0000000000003244
Biomarker-Based Risk Stratification in Pediatric Sepsis From a Low-Middle Income Country
Abstract
Objectives: Most biomarker studies of sepsis originate from high-income countries, whereas mortality risk is higher in low- and middle-income countries. The second version of the Pediatric Sepsis Biomarker Risk Model (PERSEVERE-II) has been validated in multiple North American PICUs for prognosis. Given differences in epidemiology, we assessed the performance of PERSEVERE-II in septic children from Pakistan, a low-middle income country. Due to uncertainty regarding how well PERSEVERE-II would perform, we also assessed the utility of other select biomarkers reflecting endotheliopathy, coagulopathy, and lung injury.
Design: Prospective cohort study.
Setting: PICU in Aga Khan University Hospital in Karachi, Pakistan.
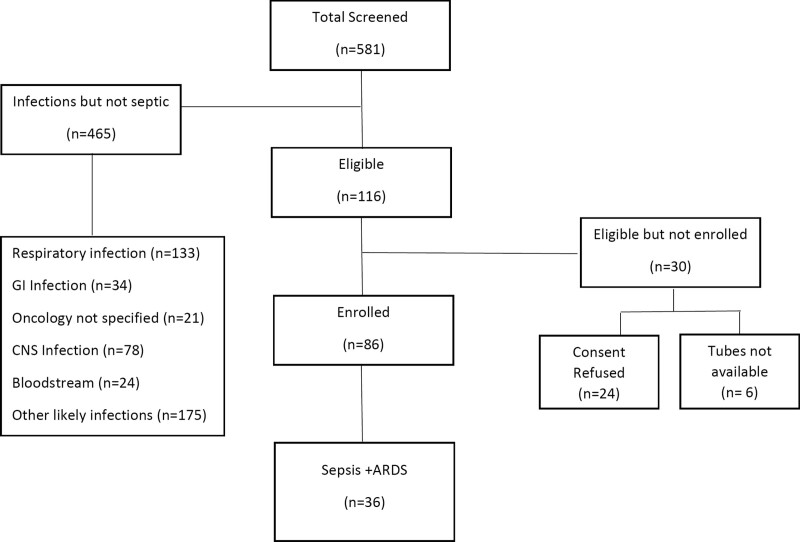
Patients: Children (< 18 yr old) meeting pediatric modifications of adult Sepsis-3 criteria between November 2020 and February 2022 were eligible.
Interventions: None.
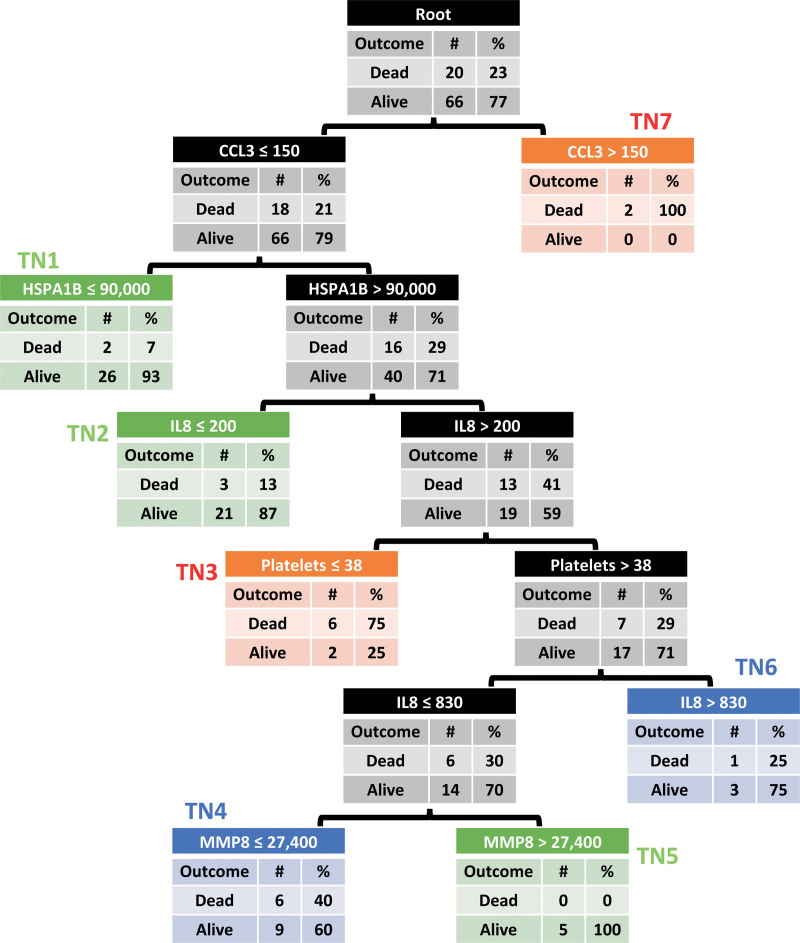
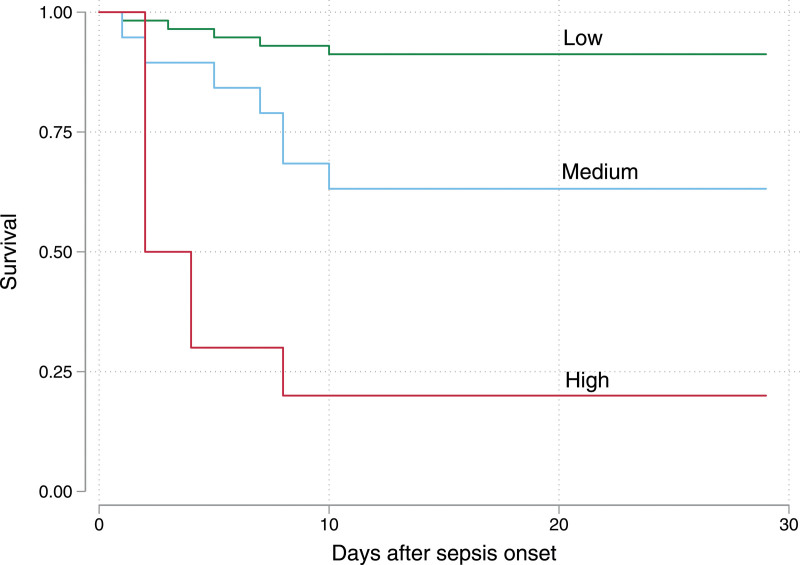
Measurements and main results: Plasma was collected within 24 hours of admission and biomarkers quantified. The area under the receiver operating characteristic curve for PERSEVERE-II to discriminate 28-day mortality was determined. Additional biomarkers were compared between survivors and nonsurvivors and between subjects with and without acute respiratory distress syndrome. In 86 subjects (20 nonsurvivors, 23%), PERSEVERE-II discriminated mortality (area under the receiver operating characteristic curve, 0.83; 95% CI, 0.72-0.94) and stratified the cohort into low-, medium-, and high-risk of mortality. Biomarkers reflecting endotheliopathy (angiopoietin 2, intracellular adhesion molecule 1) increased across worsening risk strata. Angiopoietin 2, soluble thrombomodulin, and plasminogen activator inhibitor 1 were higher in nonsurvivors, and soluble receptor for advanced glycation end-products and surfactant protein D were higher in children meeting acute respiratory distress syndrome criteria.
Conclusions: PERSEVERE-II performs well in septic children from Aga Khan University Hospital, representing the first validation of PERSEVERE-II in a low-middle income country. Patients possessed a biomarker profile comparable to that of sepsis from high-income countries, suggesting that biomarker-based enrichment strategies may be effective in this setting.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Drs. Famularo’s, Kazi’s, Parkar’s, Thompson’s, and Yehya’s institutions received funding from the National Heart, Lung, and Blood Institute. Drs. Kazi, Parkar, Thompson, and Yehya received support for article research from the National Institutes of Health. Drs. Parkar’s and Yehya’s institutions received funding from Pfizer outside of the scope of this work. Dr. Thomas received funding from Bayer AG. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, et al. : The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir Med. 2018; 6:223–230 - PubMed
-
- Black RE, Cousens S, Johnson HL, et al. ; Child Health Epidemiology Reference Group of WHO and UNICEF: Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet. 2010; 375:1969–1987 - PubMed
-
- Liu L, Oza S, Hogan D, et al. : Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet. 2015; 385:430–440 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
