

Commercial Insurance Rates and Coding for Lymphedema Procedures: The Current State of Confusion and Need for Consensus
- PMID: 37092977
- PMCID: PMC11240848
- DOI: 10.1097/PRS.0000000000010591
Commercial Insurance Rates and Coding for Lymphedema Procedures: The Current State of Confusion and Need for Consensus
Abstract
Background: Surgical treatment of lymphedema has outpaced coding paradigms. In the setting of ambiguity regarding coding for physiologic procedures [lymphovenous bypass (LVB) and vascularized lymph node transplant (VLNT)], we hypothesized that there would be variation in commercial reimbursement based on coding pattern.
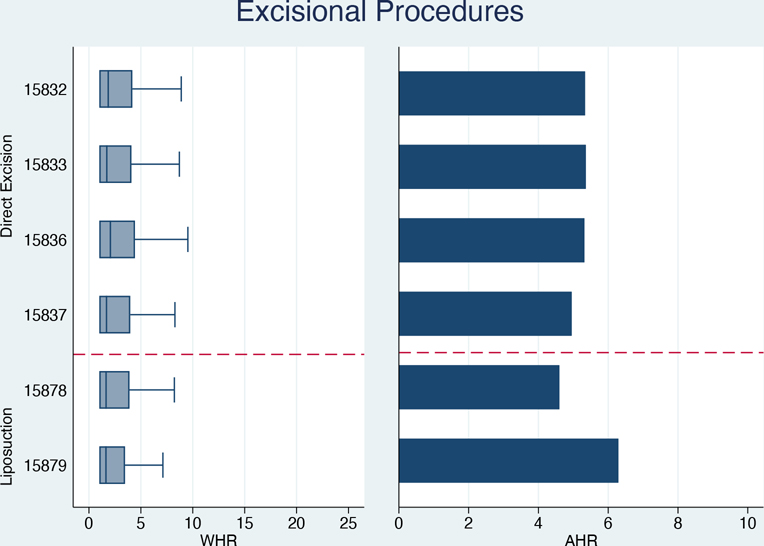
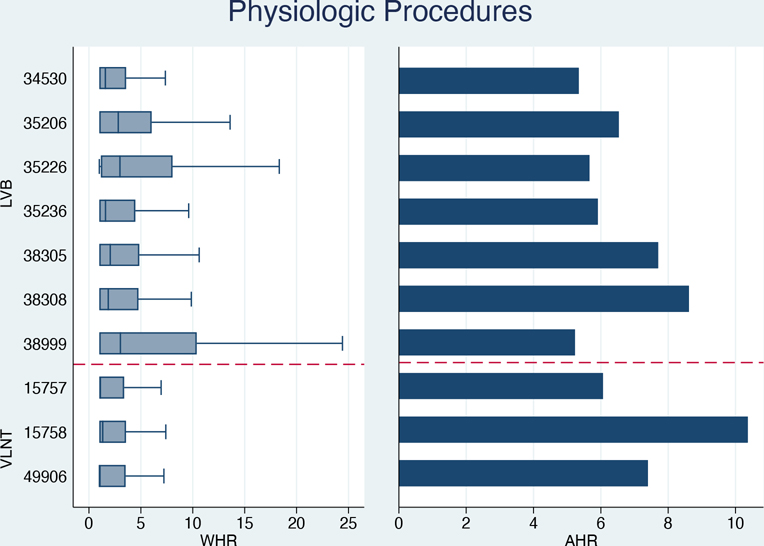
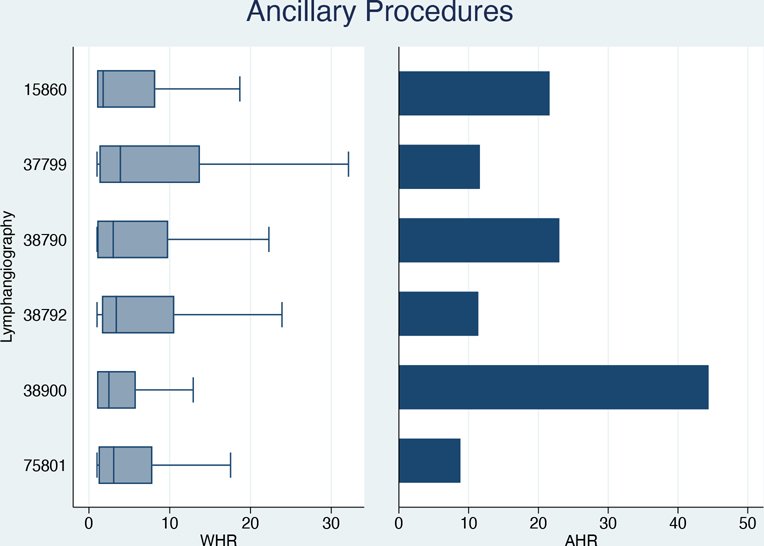
Methods: The authors performed a cross-sectional analysis of 2021 nationwide hospital pricing data for 21 CPT codes encompassing excisional (direct excision, liposuction), physiologic (LVB, VLNT), and ancillary (lymphangiography) procedures. Within-hospital ratios (WHRs) and across-hospital ratios (AHRs) for adjusted commercial rates per CPT code quantified price variation. Mixed effects linear regression modeled associations of commercial rate with public payer (Medicare and Medicaid), self-pay, and chargemaster rates.
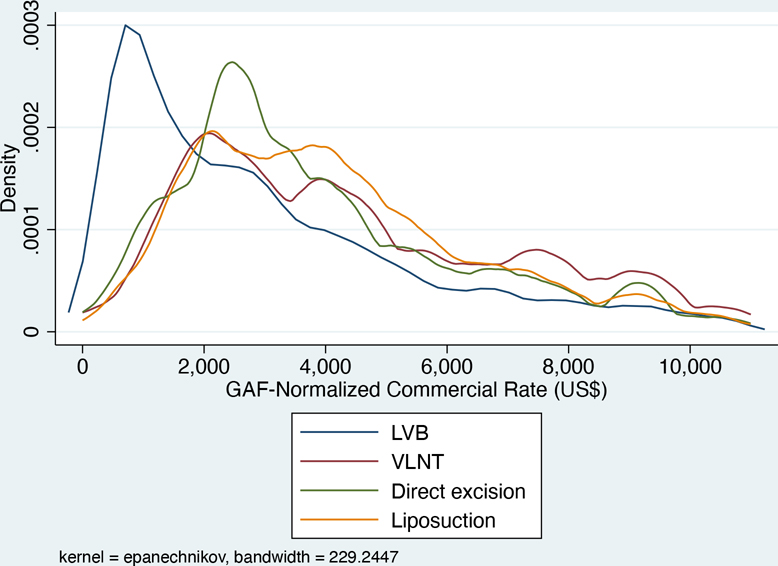
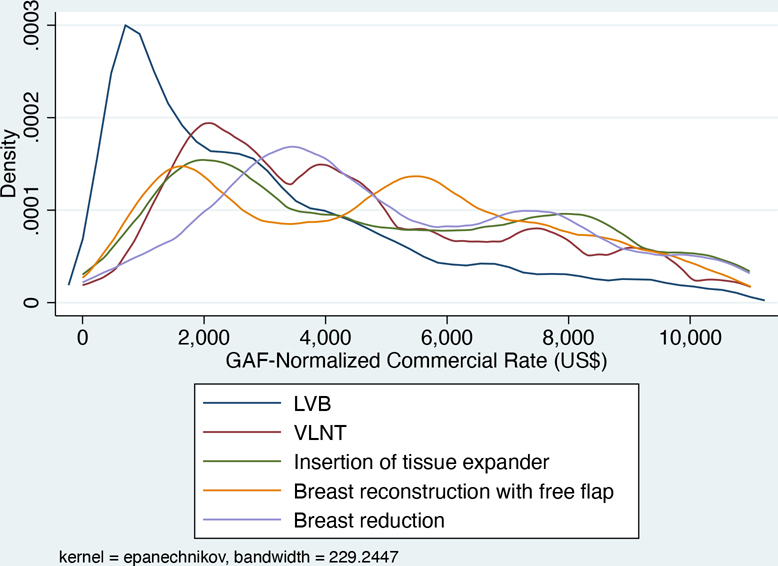
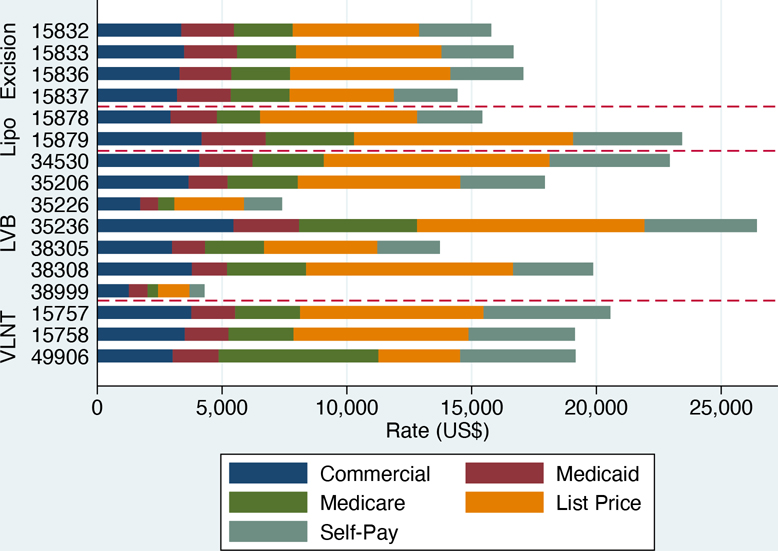
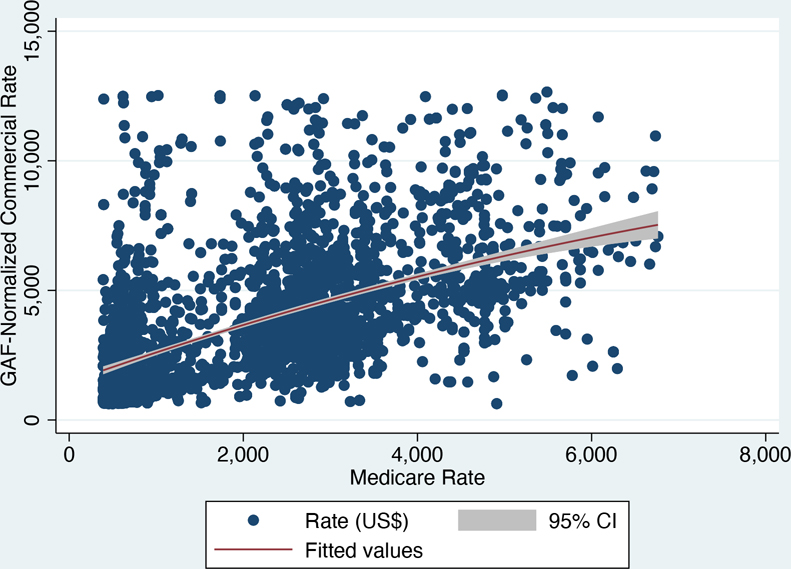
Results: A total of 270,254 commercial rates, including 95,774 rates for physiologic procedures, were extracted from 2863 hospitals. Lymphangiography codes varied most in commercial price (WHR, 1.76 to 3.89; AHR, 8.12 to 44.38). For physiologic codes, WHRs ranged from 1.01 (VLNT; free omental flap) to 3.03 (LVB; unlisted lymphatic procedure), and AHRs ranged from 5.23 (LVB; lymphatic channel incision) to 10.36 (LVB; unlisted lymphatic procedure). Median adjusted commercial rates for excisional procedures ($3635.84) were higher than for physiologic procedures ($2560.40; P < 0.001). Commercial rate positively correlated with Medicare rate for all physiologic codes combined, although regression coefficients varied by code.
Conclusions: Commercial payer-negotiated rates for physiologic procedures were highly variable both within and across hospitals, reflective of variation in CPT codes. Physiologic procedures may be undervalued relative to excisional procedures. Consistent coding nomenclature should be developed for physiologic and ancillary procedures.
Copyright © 2023 by the American Society of Plastic Surgeons.
Figures
Similar articles
-
Outcomes analysis of microsurgical physiologic lymphatic procedures for the upper extremity from the United States National Surgical Quality Improvement Program.Microsurgery. 2022 May;42(4):305-311. doi: 10.1002/micr.30844. Epub 2021 Nov 23. Microsurgery. 2022. PMID: 34812535
-
Combined Approach to Surgical Treatment of Lymphedema.Lymphat Res Biol. 2021 Feb;19(1):23-24. doi: 10.1089/lrb.2020.0098. Epub 2020 Nov 23. Lymphat Res Biol. 2021. PMID: 33226911
-
[Lympho-reconstructive microsurgery for secondary lymphedema: Consensus of the German-Speaking Society for Microsurgery of Peripheral Nerves and Vessels (DAM) on indication, diagnostic and therapy by lymphovenous anastomosis (LVA) and vascularized lymph node transfer (VLNT)].Handchir Mikrochir Plast Chir. 2019 Dec;51(6):424-433. doi: 10.1055/a-0874-2212. Epub 2019 May 8. Handchir Mikrochir Plast Chir. 2019. PMID: 31067594 German.
-
Surgical Treatment of Lymphedema.Plast Reconstr Surg. 2019 Sep;144(3):738-758. doi: 10.1097/PRS.0000000000005993. Plast Reconstr Surg. 2019. PMID: 31461041 Review.
-
Combined deep inferior epigastric artery perforator flap with vascularized groin lymph node transplant for treatment of breast cancer-related lymphedema.Gland Surg. 2021 Jan;10(1):460-468. doi: 10.21037/gs.2020.02.14. Gland Surg. 2021. PMID: 33634003 Free PMC article. Review.
Cited by
-
Lower Commercial Rates for Breast Surgical Procedures are Associated with Socioeconomic Disadvantage: A Transparency in Coverage Analysis.Ann Surg Oncol. 2025 May;32(5):3695-3704. doi: 10.1245/s10434-024-16738-z. Epub 2024 Dec 24. Ann Surg Oncol. 2025. PMID: 39719512
-
Discussion: Commercial Insurance Rates and Coding for Lymphedema Procedures: The Current State of Confusion and Need for Consensus.Plast Reconstr Surg. 2024 Jan 1;153(1):256-257. doi: 10.1097/PRS.0000000000010963. Epub 2023 Dec 21. Plast Reconstr Surg. 2024. PMID: 38127452 Free PMC article. No abstract available.
-
Modern approaches to lymphatic surgery: a narrative review.Transl Breast Cancer Res. 2025 Jan 21;6:6. doi: 10.21037/tbcr-24-49. eCollection 2025. Transl Breast Cancer Res. 2025. PMID: 39980814 Free PMC article. Review.
References
-
- Charles H Elephantiasis of the Leg. In: Latham A, English T, eds. A System of Treatment. Vol 3. Churchill; 1912.
-
- Sistrunk W Modification of the Operation for Elephantiasis. JAMA. 1918;71:800–803.
-
- Schaverien MV, Dayan JH. Key Topic: Patient Selection and Evidence-Based Algorithmic Approach to Surgical Management of Lymphedema. In: Schaverien MV, Dayan JH, eds. Multimodal Management of Upper and Lower Extremity Lymphedema. Springer International Publishing; 2022:47–52.
-
- Brorson H Liposuction in Arm Lymphedema Treatment. Scand J Surg. 2003;92(4):287–295. - PubMed
-
- Chang DW, Dayan J, Greene AK, et al. Surgical Treatment of Lymphedema: A Systematic Review and Meta-Analysis of Controlled Trials. Results of a Consensus Conference. Plastic & Reconstructive Surgery. 2021;147(4):975–993. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
