

SARS-CoV-2 Outbreak Investigation Using Contact Tracing and Whole-Genome Sequencing in an Ontario Tertiary Care Hospital
- PMID: 37093060
- PMCID: PMC10269621
- DOI: 10.1128/spectrum.01900-22
SARS-CoV-2 Outbreak Investigation Using Contact Tracing and Whole-Genome Sequencing in an Ontario Tertiary Care Hospital
Abstract
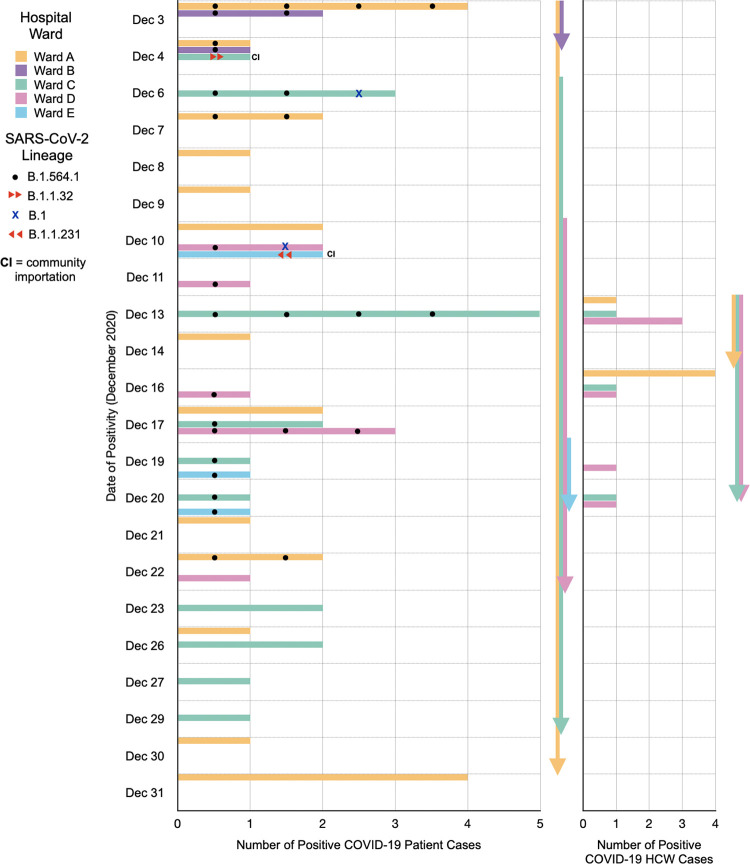
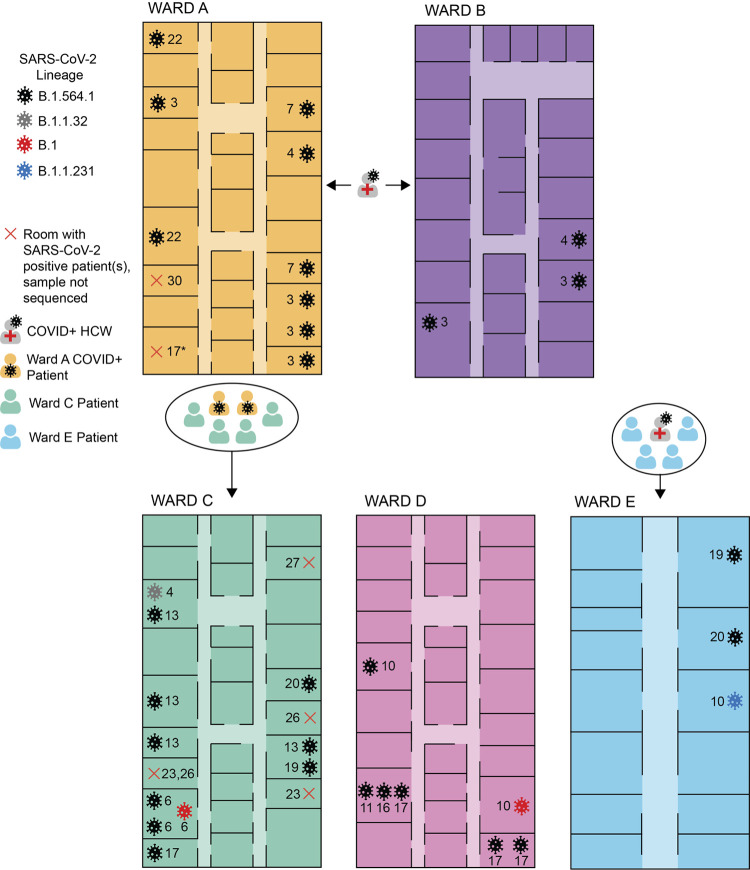
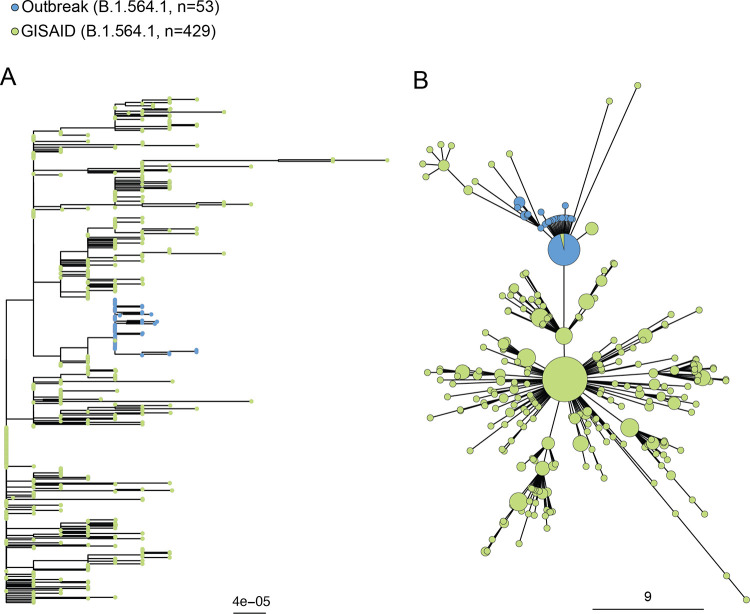
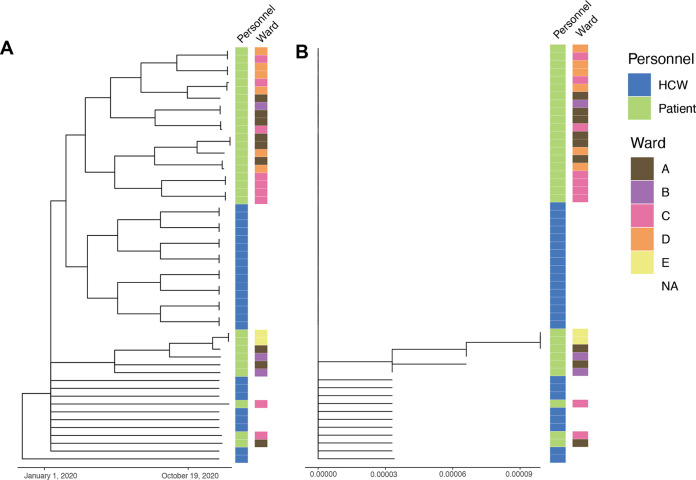
Genomic epidemiology can facilitate an understanding of evolutionary history and transmission dynamics of a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) outbreak. We used next-generation sequencing techniques to study SARS-CoV-2 genomes isolated from patients and health care workers (HCWs) across five wards of a Canadian hospital with an ongoing SARS-CoV-2 outbreak. Using traditional contact tracing methods, we show transmission events between patients and HCWs, which were also supported by the SARS-CoV-2 lineage assignments. The outbreak predominantly involved SARS-CoV-2 B.1.564.1 across all five wards, but we also show evidence of community introductions of lineages B.1, B.1.1.32, and B.1.231, falsely assumed to be outbreak related. Altogether, our study exemplifies the value of using contact tracing in combination with genomic epidemiology to understand the transmission dynamics and genetic underpinnings of a SARS-CoV-2 outbreak. IMPORTANCE Our manuscript describes a SARS-CoV-2 outbreak investigation in an Ontario tertiary care hospital. We use traditional contract tracing paired with whole-genome sequencing to facilitate an understanding of the evolutionary history and transmission dynamics of this SARS-CoV-2 outbreak in a clinical setting. These advancements have enabled the incorporation of phylogenetics and genomic epidemiology into the understanding of clinical outbreaks. We show that genomic epidemiology can help to explore the genetic evolution of a pathogen in real time, enabling the identification of the index case and helping understand its transmission dynamics to develop better strategies to prevent future spread of SARS-CoV-2 in congregate, clinical settings such as hospitals.
Keywords: COVID-19; Canada; DNA sequencing; SARS-CoV-2; contact tracing; genomics; hospital; outbreak.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Comprehensive contact tracing during an outbreak of alpha-variant SARS-CoV-2 in a rural community reveals less viral genomic diversity and higher household secondary attack rates than expected.mSphere. 2024 Aug 28;9(8):e0011424. doi: 10.1128/msphere.00114-24. Epub 2024 Aug 7. mSphere. 2024. PMID: 39109863 Free PMC article.
-
Nosocomial Outbreak of SARS-CoV-2 in a "Non-COVID-19" Hospital Ward: Virus Genome Sequencing as a Key Tool to Understand Cryptic Transmission.Viruses. 2021 Apr 1;13(4):604. doi: 10.3390/v13040604. Viruses. 2021. PMID: 33916205 Free PMC article.
-
Lessons learned: use of WGS in real-time investigation of suspected intrahospital SARS-CoV-2 outbreaks.J Hosp Infect. 2023 Jan;131:81-88. doi: 10.1016/j.jhin.2022.10.003. Epub 2022 Oct 29. J Hosp Infect. 2023. PMID: 36404573 Free PMC article.
-
Nosocomial Coronavirus Disease Outbreak Containment, Hanoi, Vietnam, March-April 2020.Emerg Infect Dis. 2021 Jan;27(1):10-7. doi: 10.3201/eid2701.202656. Epub 2020 Nov 18. Emerg Infect Dis. 2021. PMID: 33207153 Free PMC article. Review.
-
Perfect as the enemy of good: tracing transmissions with low-sensitivity tests to mitigate SARS-CoV-2 outbreaks.Lancet Microbe. 2021 May;2(5):e219-e224. doi: 10.1016/S2666-5247(21)00004-5. Epub 2021 Mar 12. Lancet Microbe. 2021. PMID: 33748803 Free PMC article. Review.
Cited by
-
Contact tracing strategies for infectious diseases: A systematic literature review.PLOS Glob Public Health. 2025 May 9;5(5):e0004579. doi: 10.1371/journal.pgph.0004579. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 40343962 Free PMC article.
-
The utility of whole-genome sequencing to inform epidemiologic investigations of SARS-CoV-2 clusters in acute-care hospitals.Infect Control Hosp Epidemiol. 2024 Feb;45(2):144-149. doi: 10.1017/ice.2023.274. Epub 2023 Dec 22. Infect Control Hosp Epidemiol. 2024. PMID: 38130169 Free PMC article.
References
-
- Rabaan AA, Al-Ahmed SH, Sah R, Al-Tawfiq JA, Haque S, Harapan H, Arteaga-Livias K, Aldana DKB, Kumar P, Dhama K, Rodriguez-Morales AJ. 2020. Genomic epidemiology and recent update on nucleic acid–based diagnostics for COVID-19. Curr Trop Med Rep 7:113–119. doi:10.1007/s40475-020-00212-3. - DOI - PMC - PubMed
-
- Wenlock RD, Tausan M, Mann R, Garr W, Preston R, Arnold A, Hoban J, Webb L, Quick C, Beckett A, Loveson K, Glaysher S, Elliott S, Malone C, Cogger B, Easton L, Robson SC, Hassan-Ibrahim MO, Sargent C. COVID-19 Genomics UK (COG-UK) Consortium. 2021. Nosocomial or not? A combined epidemiological and genomic investigation to understand hospital-acquired COVID-19 infection on an elderly care ward. Infect Prev Pract 3:100165. doi:10.1016/j.infpip.2021.100165. - DOI - PMC - PubMed
-
- Lumley SF, Constantinides B, Sanderson N, Rodger G, Street TL, Swann J, Chau KK, O'Donnell D, Warren F, Hoosdally S, O'Donnell A-M, Walker TM, Stoesser NE, Butcher L, Peto TE, Crook DW, Jeffery K, Matthews PC, Eyre DW. OUH Infection Prevention and Control Team. 2021. Epidemiological data and genome sequencing reveals that nosocomial transmission of SARS-CoV-2 is underestimated and mostly mediated by a small number of highly infectious individuals. J Infect 83:473–482. doi:10.1016/j.jinf.2021.07.034. - DOI - PMC - PubMed
-
- Meijer SE, Harel N, Ben-Ami R, Nahari M, Yakubovsky M, Oster HS, Kolomansky A, Halutz O, Laskar O, Henig O, Stern A, Paran Y. 2021. Unraveling a nosocomial outbreak of COVID-19: the role of whole-genome sequence analysis. Open Forum Infect Dis 8:ofab120. doi:10.1093/ofid/ofab120. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
