

Simultaneous resection of colorectal cancer and synchronous liver metastases: what determines the risk of unfavorable outcomes? An international multicenter retrospective cohort study
- PMID: 37093069
- PMCID: PMC10389225
- DOI: 10.1097/JS9.0000000000000068
Simultaneous resection of colorectal cancer and synchronous liver metastases: what determines the risk of unfavorable outcomes? An international multicenter retrospective cohort study
Abstract
Background: The use of a simultaneous resection (SIMR) in patients with synchronous colorectal liver metastases (sCRLM) has increased over the past decades. However, it remains unclear when a SIMR is beneficial and when it should be avoided. The aim of this retrospective cohort study was therefore to compare the outcomes of a SIMR for sCRLM in different settings, and to assess which factors are independently associated with unfavorable outcomes.
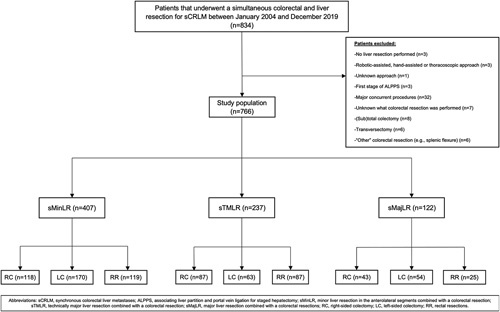
Methods: To perform this retrospective cohort study, patients with sCRLM undergoing SIMR (2004-2019) were extracted from an international multicenter database, and their outcomes were compared after stratification according to the type of liver and colorectal resection performed. Factors associated with unfavorable outcomes were identified through multivariable logistic regression.
Results: Overall, 766 patients were included, encompassing colorectal resections combined with a major liver resection (n=122), minor liver resection in the anterolateral (n=407), or posterosuperior segments ('Technically major', n=237). Minor and technically major resections, compared to major resections, were more often combined with a rectal resection (29.2 and 36.7 vs. 20.5%, respectively, both P=0.003) and performed fully laparoscopic (22.9 and 23.2 vs. 6.6%, respectively, both P = 0.003). Major and technically major resections, compared to minor resections, were more often associated with intraoperative transfusions (42.9 and 38.8 vs. 20%, respectively, both P = 0.003) and unfavorable incidents (9.6 and 9.8 vs. 3.3%, respectively, both P≤0.063). Major resections were associated, compared to minor and technically major resections, with a higher overall morbidity rate (64.8 vs. 50.4 and 49.4%, respectively, both P≤0.024) and a longer length of stay (12 vs. 10 days, both P≤0.042). American Society of Anesthesiologists grades ≥3 [adjusted odds ratio (aOR): 1.671, P=0.015] and undergoing a major liver resection (aOR: 1.788, P=0.047) were independently associated with an increased risk of severe morbidity, while undergoing a left-sided colectomy was associated with a decreased risk (aOR: 0.574, P=0.013).
Conclusions: SIMR should primarily be reserved for sCRLM patients in whom a minor or technically major liver resection would suffice and those requiring a left-sided colectomy. These findings should be confirmed by randomized studies comparing SIMR with staged resections.
Trial registration: ClinicalTrials.gov NCT05475041.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no related conflicts of interest to declare.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021;71:209–249. - PubMed
-
- Horn SR, Stoltzfus KC, Lehrer EJ, et al. Epidemiology of liver metastases. Cancer Epidemiol 2020;67:101760. - PubMed
-
- Adam R, de Gramont A, Figueras J, et al. Managing synchronous liver metastases from colorectal cancer: a multidisciplinary international consensus. Cancer Treat Rev 2015;41:729–741. - PubMed
-
- Lambert LA, Colacchio TA, Barth RJ. Interval hepatic resection of colorectal metastases improves patient selection. Arch Surg 2000;135:473–480. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
