

Characteristics of Progressive Multifocal Leukoencephalopathy Associated With Sarcoidosis Without Therapeutic Immune Suppression
- PMID: 37093609
- PMCID: PMC10126944
- DOI: 10.1001/jamaneurol.2023.0841
Characteristics of Progressive Multifocal Leukoencephalopathy Associated With Sarcoidosis Without Therapeutic Immune Suppression
Abstract
Importance: Progressive multifocal leukoencephalopathy can occur in the context of systemic sarcoidosis (S-PML) in the absence of therapeutic immune suppression and can initially be mistaken for neurosarcoidosis or other complications of sarcoidosis. Earlier recognition of S-PML could lead to more effective treatment of the disease.
Objective: To describe characteristics of patients with S-PML.
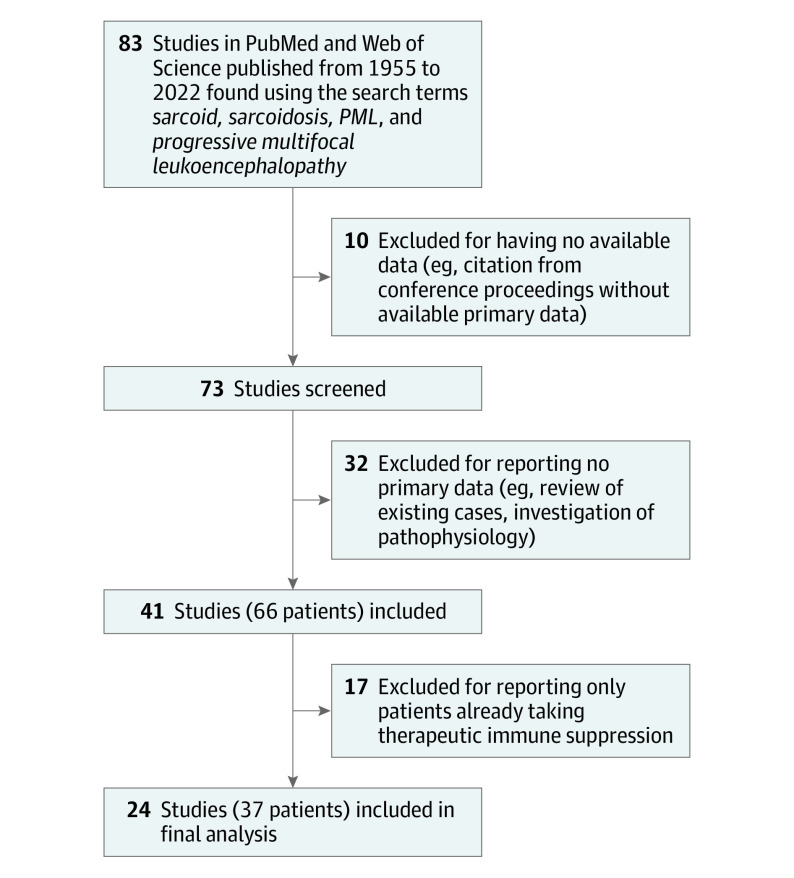
Design, setting, and participants: For this case series, records from 8 academic medical centers in the United States were reviewed from 2004 to 2022. A systematic review of literature from 1955 to 2022 yielded data for additional patients. Included were patients with S-PML who were not receiving therapeutic immune suppression. The median follow-up time for patients who survived the acute range of illness was 19 months (range, 2-99). Data were analyzed in February 2023.
Exposures: Sarcoidosis without active therapeutic immune suppression.
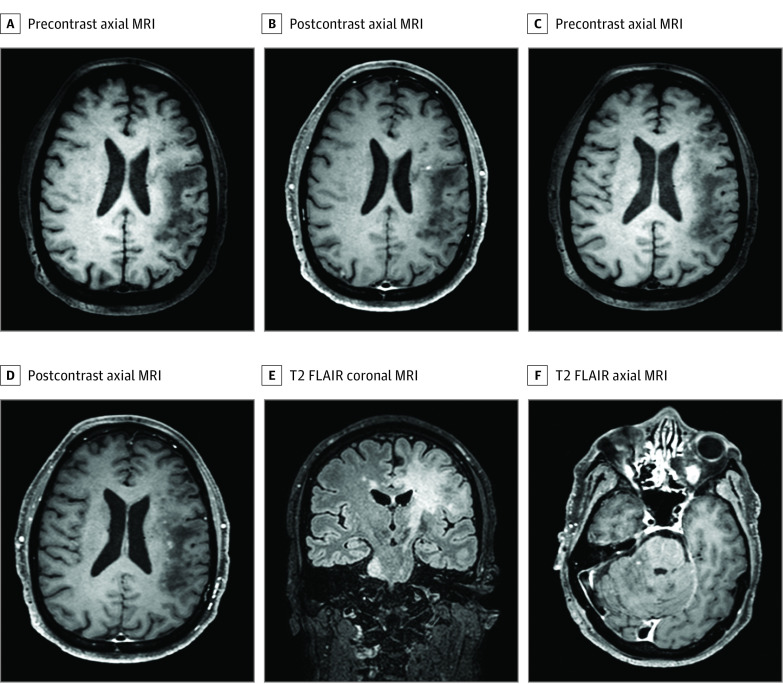
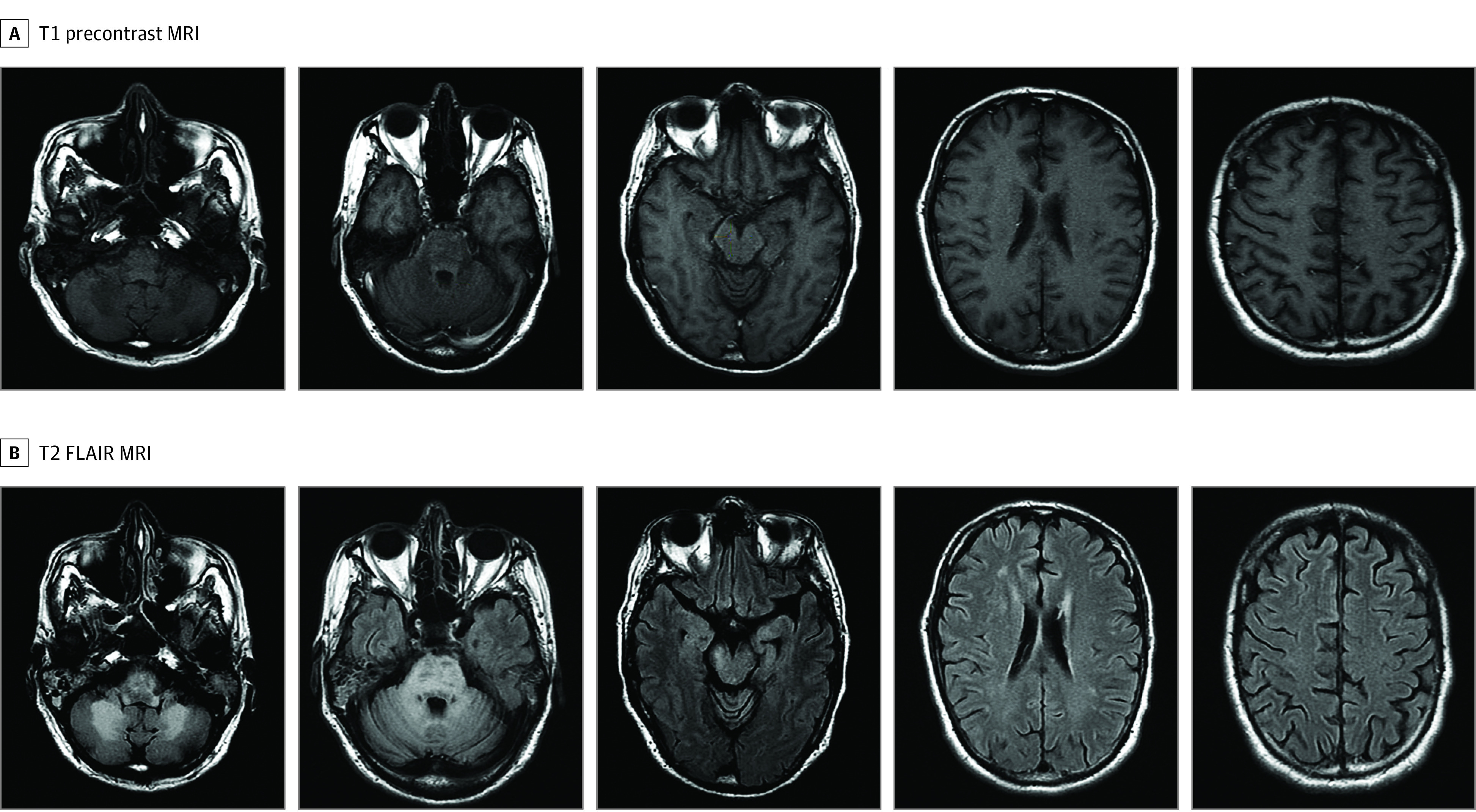
Main outcomes and measures: Clinical, laboratory, and radiographic features of patients with S-PML.
Results: Twenty-one patients with S-PML not receiving therapeutic immune suppression were included in this study, and data for 37 patients were collected from literature review. The median age of the 21 study patients was 56 years (range, 33-72), 4 patients (19%) were female, and 17 (81%) were male. The median age of the literature review patients was 49 years (range, 21-74); 12 of 34 patients (33%) with reported sex were female, and 22 (67%) were male. Nine of 21 study patients (43%) and 18 of 31 literature review patients (58%) had simultaneous presentation of systemic sarcoidosis and PML. Six of 14 study patients (43%) and 11 of 19 literature review patients (58%) had a CD4+ T-cell count greater than 200/μL. In 2 study patients, a systemic flare of sarcoidosis closely preceded S-PML development. Ten of 17 study patients (59%) and 21 of 35 literature review patients (60%) died during the acute phase of illness. No meaningful predictive differences were found between patients who survived S-PML and those who did not.
Conclusions and relevance: In this case series, patients with sarcoidosis developed PML in the absence of therapeutic immune suppression, and peripheral blood proxies of immune function were often only mildly abnormal. Systemic sarcoidosis flares may rarely herald the onset of S-PML. Clinicians should consider PML in any patient with sarcoidosis and new white matter lesions on brain magnetic resonance imaging.
Conflict of interest statement
Figures
References
-
- Astrom KE, Mancall EL, Richardson EP Jr. Progressive multifocal leuko-encephalopathy; a hitherto unrecognized complication of chronic lymphatic leukaemia and Hodgkin’s disease. Brain. 1958;81(1):93-111. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
