

Preterm Birth, Small for Gestational Age, and Large for Gestational Age and the Risk of Atrial Fibrillation Up to Middle Age
- PMID: 37093612
- PMCID: PMC10126943
- DOI: 10.1001/jamapediatrics.2023.0083
Preterm Birth, Small for Gestational Age, and Large for Gestational Age and the Risk of Atrial Fibrillation Up to Middle Age
Abstract
Importance: Adverse birth outcomes, including preterm birth, small for gestational age (SGA), and large for gestational age (LGA) are associated with increased risks of hypertension, ischemic heart disease, stroke, and heart failure, but knowledge regarding their associations with atrial fibrillation (AF) is limited and inconsistent.
Objective: To investigate whether preterm birth, SGA, or LGA are associated with increased risks of AF later in life.
Design, setting, and participants: This multinational cohort study included Danish, Swedish, and Finnish national health registries. Live singleton births in Denmark from 1978 through 2016, in Sweden from 1973 through 2014, and in Finland from 1987 through 2014, who were followed up until December 31, 2016, in Denmark, December 31, 2021, in Sweden, and December 31, 2014, in Finland were included. Data analyses were performed between January 2021 and August 2022.
Exposures: Preterm birth (less than 37 gestational weeks), SGA (less than 10th percentile birth weight for gestational age), and LGA (more than 90th percentile birth weight for gestational age) identified from medical birth registers.
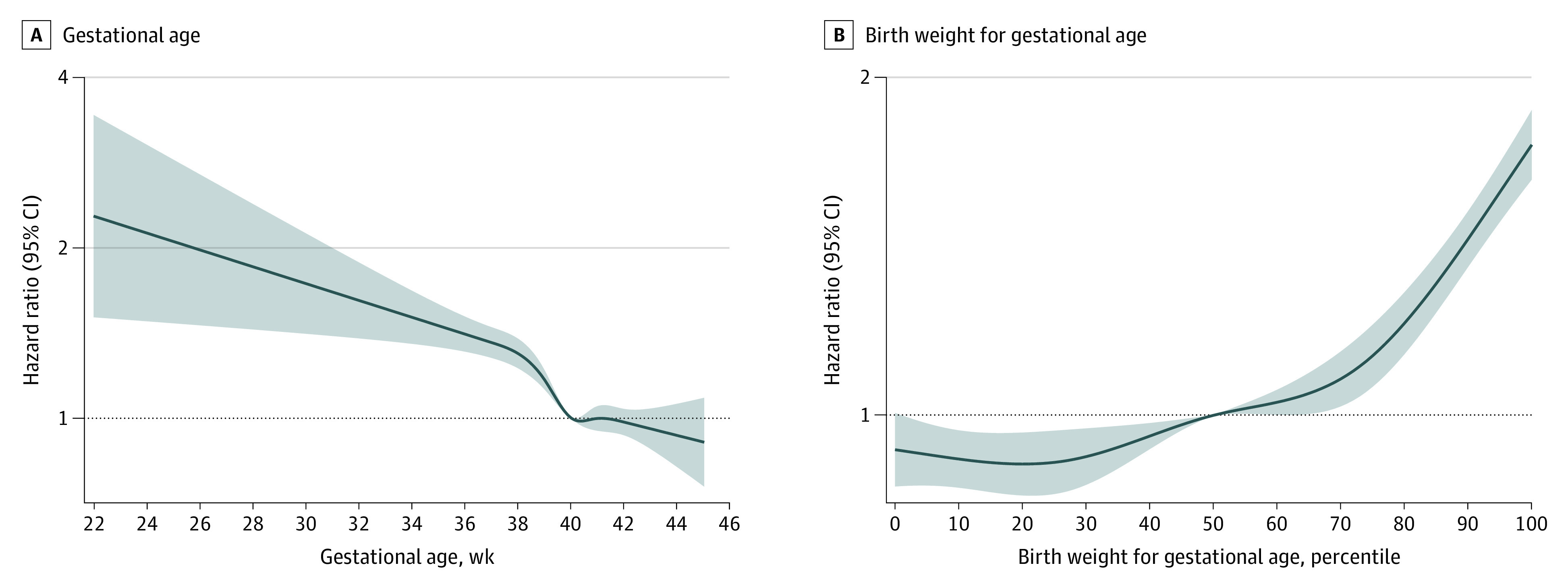
Main outcomes and measures: Diagnosis of AF obtained from nationwide inpatient and outpatient registers. The study team ran multivariable Cox proportional hazard models and flexible parametric survival models to estimate hazard ratios (HRs) and 95% CIs for AF according to preterm birth, SGA, and LGA. Sibling analyses were conducted to control for unmeasured familial factors.
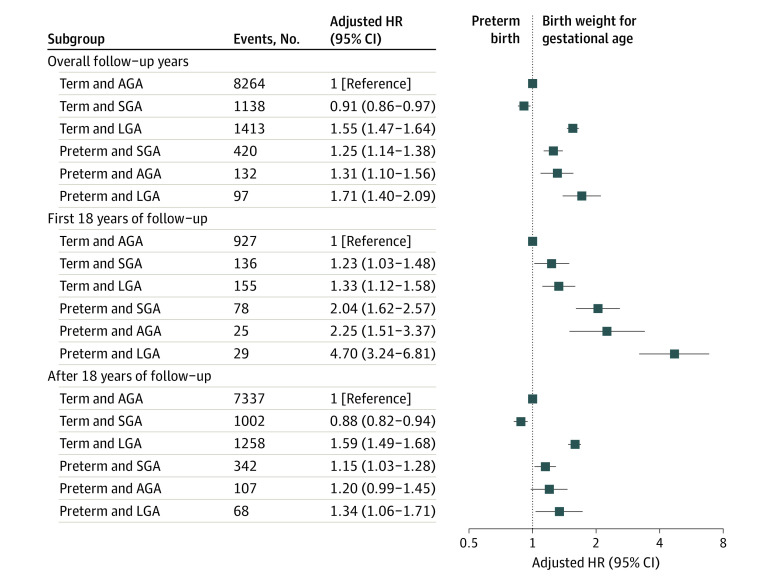
Results: The cohort included 8 012 433 study participants (maximum age, 49 years; median age, 21 years; male, 51.3%). In 174.4 million person-years of follow-up, 11 464 participants had a diagnosis of AF (0.14%; median age, 29.3 years). Preterm birth and LGA were associated with increased AF risk in both the full population cohort and in the sibling analyses; the multivariate HRs from the cohort analyses were 1.30 (95% CI, 1.18-1.42) and 1.55 (95% CI, 1.46-1.63), respectively. Preterm birth was more strongly associated with AF in childhood than in adulthood. Children born SGA had an increased risk of AF in the first 18 years of life but not afterwards.
Conclusions and relevance: Preterm births and LGA births were associated with increased risks of AF up to middle age independently of familial confounding factors. Individuals born SGA had an increased AF risk only during childhood.
Conflict of interest statement
Figures

References
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263-272. doi:10.1378/chest.09-1584 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
