

Identification of pregnancies and their outcomes in healthcare claims data, 2008-2019: An algorithm
- PMID: 37093890
- PMCID: PMC10124843
- DOI: 10.1371/journal.pone.0284893
Identification of pregnancies and their outcomes in healthcare claims data, 2008-2019: An algorithm
Abstract
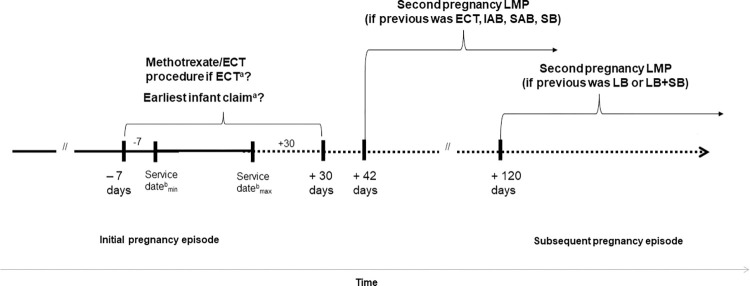
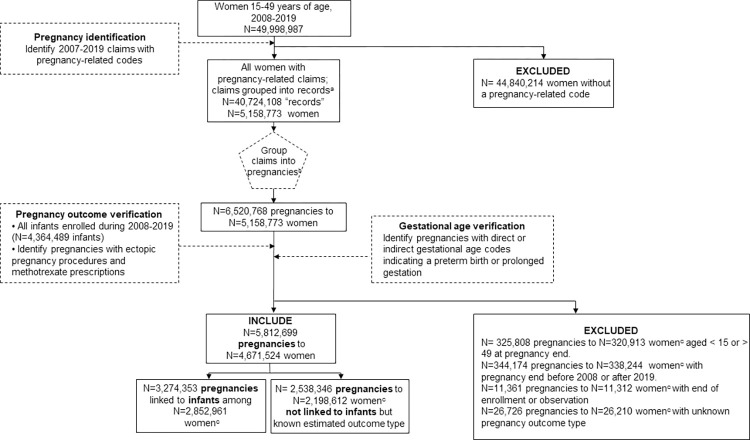
Pregnancy is a condition of broad interest across many medical and health services research domains, but one not easily identified in healthcare claims data. Our objective was to establish an algorithm to identify pregnant women and their pregnancies in claims data. We identified pregnancy-related diagnosis, procedure, and diagnosis-related group codes, accounting for the transition to International Statistical Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) diagnosis and procedure codes, in health encounter reporting on 10/1/2015. We selected women in Merative MarketScan commercial databases aged 15-49 years with pregnancy-related claims, and their infants, during 2008-2019. Pregnancies, pregnancy outcomes, and gestational ages were assigned using the constellation of service dates, code types, pregnancy outcomes, and linkage to infant records. We describe pregnancy outcomes and gestational ages, as well as maternal age, census region, and health plan type. In a sensitivity analysis, we compared our algorithm-assigned date of last menstrual period (LMP) to fertility procedure-based LMP (date of procedure + 14 days) among women with embryo transfer or insemination procedures. Among 5,812,699 identified pregnancies, most (77.9%) were livebirths, followed by spontaneous abortions (16.2%); 3,274,353 (72.2%) livebirths could be linked to infants. Most pregnancies were among women 25-34 years (59.1%), living in the South (39.1%) and Midwest (22.4%), with large employer-sponsored insurance (52.0%). Outcome distributions were similar across ICD-9 and ICD-10 eras, with some variation in gestational age distribution observed. Sensitivity analyses supported our algorithm's framework; algorithm- and fertility procedure-derived LMP estimates were within a week of each other (mean difference: -4 days [IQR: -13 to 6 days]; n = 107,870). We have developed an algorithm to identify pregnancies, their gestational age, and outcomes, across ICD-9 and ICD-10 eras using administrative data. This algorithm may be useful to reproductive health researchers investigating a broad range of pregnancy and infant outcomes.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures
References
-
- Ailes EC, Simeone RM, Dawson AL, Petersen EE, Gilboa SM. Using insurance claims data to identify and estimate critical periods in pregnancy: An application to antidepressants. Birth Defects Res A Clin Mol Teratol. 2016;106(11):927–34. Epub 2016/11/29. doi: 10.1002/bdra.23573 ; PubMed Central PMCID: PMC5225464. - DOI - PMC - PubMed
-
- Blotiere PO, Weill A, Dalichampt M, Billionnet C, Mezzarobba M, Raguideau F, et al.. Development of an algorithm to identify pregnancy episodes and related outcomes in health care claims databases: An application to antiepileptic drug use in 4.9 million pregnant women in France. Pharmacoepidemiol Drug Saf. 2018;27(7):763–70. Epub 2018/05/16. doi: 10.1002/pds.4556 ; PubMed Central PMCID: PMC6055607. - DOI - PMC - PubMed
-
- Korelitz JJ, McNally DL, Masters MN, Li SX, Xu Y, Rivkees SA. Prevalence of thyrotoxicosis, antithyroid medication use, and complications among pregnant women in the United States. Thyroid. 2013;23(6):758–65. Epub 2012/12/01. doi: 10.1089/thy.2012.0488 ; PubMed Central PMCID: PMC3675839. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
