

Epidemiology, Outcomes, and Complement Gene Variants in Secondary Thrombotic Microangiopathies
- PMID: 37094330
- PMCID: PMC10356144
- DOI: 10.2215/CJN.0000000000000182
Epidemiology, Outcomes, and Complement Gene Variants in Secondary Thrombotic Microangiopathies
Abstract
Background: The identification of complement defects as major drivers of primary atypical hemolytic uremic syndrome (HUS) has transformed the landscape of thrombotic microangiopathies (TMAs), leading to the development of targeted therapies and better patient outcomes. By contrast, little is known about the presentation, genetics, and outcomes of TMA associated with specific diseases or conditions, also referred to as secondary TMA.
Methods: In this study, we assessed the relative incidence, clinical and genetic spectra, and long-term outcomes of secondary TMA versus other TMAs in consecutive patients hospitalized with a first episode of TMA from 2009 to 2019 at two European reference centers.
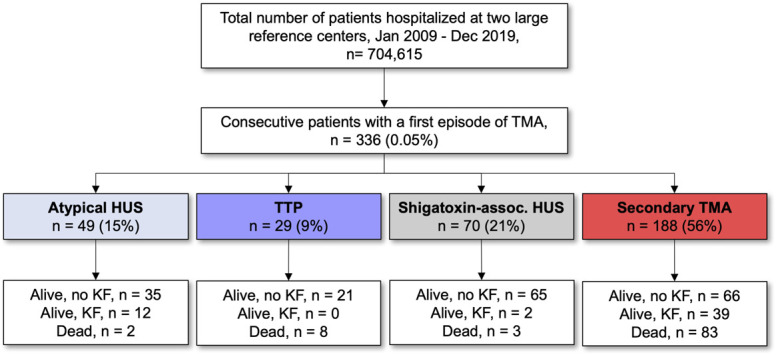
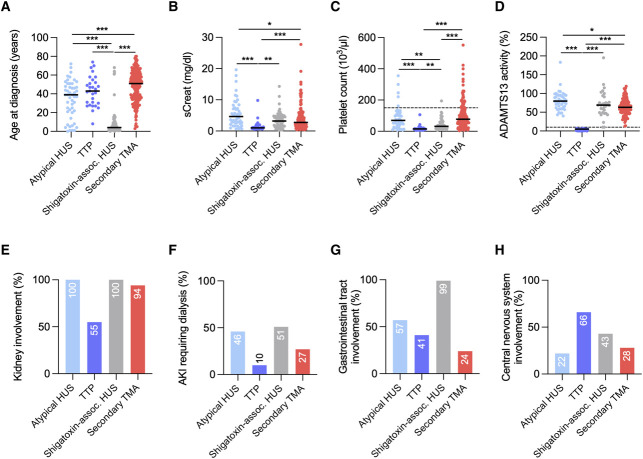
Results: During the study period, 336 patients were hospitalized with a first episode of TMA. Etiologies included atypical HUS in 49 patients (15%), thrombotic thrombocytopenic purpura (TTP) in 29 (9%), shigatoxin-associated HUS in 70 (21%), and secondary TMA in 188 (56%). The main causes of secondary TMA were hematopoietic stem-cell transplantation ( n =56, 30%), solid-organ transplantation ( n =44, 23%), and malignant hypertension ( n =25, 13%). Rare variants in complement genes were identified in 32 of 49 patients (65%) with atypical HUS and eight of 64 patients (13%) with secondary TMA; pathogenic or likely pathogenic variants were found in 24 of 49 (49%) and two of 64 (3%) of them, respectively ( P < 0.001). After a median follow-up of 1157 days, death or kidney failure occurred in 14 (29%), eight (28%), five (7%), and 121 (64%) patients with atypical HUS, TTP, shigatoxin-associated HUS, and secondary TMA, respectively. Unadjusted and adjusted Cox regressions showed that patients with secondary TMA had the highest risk of death or kidney failure (unadjusted hazard ratio [HR], 3.35; 95% confidence interval [CI], 1.85 to 6.07; P < 0.001; adjusted HR, 4.11; 95% CI, 2.00 to 8.46; P < 0.001; considering atypical HUS as reference).
Conclusions: Secondary TMAs represent the main cause of TMA and are independently associated with a high risk of death and progression to kidney failure.
Trial registration: ClinicalTrials.gov NCT04743804.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
C. Beguin reports employment with Cliniques Universitaires Saint Luc—Université catholique de Louvain. J. Bernards reports employment with ZNA Middelheim, Antwerpen, Belgium. J.-F. Cambier reports consultancy for Vifor and honoraria from AstraZeneca and Boehringer Ingelheim. K.J. Claes reports consultancy for Alexion Pharmaceuticals, Astellas, Fresenius Kabi, GSK, and Sanofi; advisory or leadership roles for Alexion, Astellas, and Fresenius Kabi; and speaker's fee for AstraZeneca and Vifor Pharma. K. Dahan reports employment with Institut de Pathologie et de Génétique de Gosselies and Universite Catholique de Louvain; consultancy for AstraZeneca and CHIESI; and advisory or leadership roles as President and a member of advisory committees for three nonprofit patient organizations: AIRG, FAPA, and Retina, and an advisory or leadership role for the Board of Directors of IPG. D. Dierickx reports employment with University Hospitals Leuven, consultancy for Sanofi Genzyme, and honoraria from Sanofi Genzyme. C. Lambert reports employment with Cliniques universitaires Saint-Luc. E. Levtchenko reports consultancy for Chiesi, KKI, and Recordati and advisory or leadership roles for Chesi, Advicenne, KKI, and Recordati. T. Meyskens reports employment with AZ Klina/AZ Voorkempen. J. Morelle reports employment with Cliniques universitaires Saint-Luc, Brussels, Belgium, and UCLouvain, Brussels, Belgium; consultancy for Alexion Pharmaceuticals, AstraZeneca, Bayer, GlaxoSmithKline, and Sanofi-Genzyme; research funding from Alexion Pharmaceuticals, AstraZeneca, and Baxter Healthcare; advisory or leadership roles for Alexion Pharmaceuticals, AstraZeneca, Bayer, Sanofi-Genzyme, and Versantis; speaker honoraria for AstraZeneca, Baxter Healthcare, and Fresenius Medical Care; funding from the National Fund for Scientific Research (FRS-FNRS, Brussels, Belgium), the Association pour l’Information et la Recherche sur les Maladies Rénales Génétiques (AIRG, Brussels, Belgium), and the Saint-Luc Foundation (Brussels, Belgium); and travel grants from Sanofi-Genzyme and Vifor Pharma. X. Poiré reports employment with Cliniques Universitaires St-Luc and consultancy for MSD and Novartis. P. Storms's spouse reports employment (currently and during the past 24 months) with Puilaetco, a Quintet Private Bank (Europe) SA Branch. Y. Zizi reports employment with Cliniques universitaires Saint-Luc. All remaining authors have nothing to disclose.
Figures


Comment in
-
Hemolytic Uremic Syndrome: A Question of Terminology.Clin J Am Soc Nephrol. 2023 Jul 1;18(7):831-833. doi: 10.2215/CJN.0000000000000198. Epub 2023 May 29. Clin J Am Soc Nephrol. 2023. PMID: 37249504 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
