

Sample-to-answer platform for the clinical evaluation of COVID-19 using a deep learning-assisted smartphone-based assay
- PMID: 37095107
- PMCID: PMC10124933
- DOI: 10.1038/s41467-023-38104-5
Sample-to-answer platform for the clinical evaluation of COVID-19 using a deep learning-assisted smartphone-based assay
Abstract
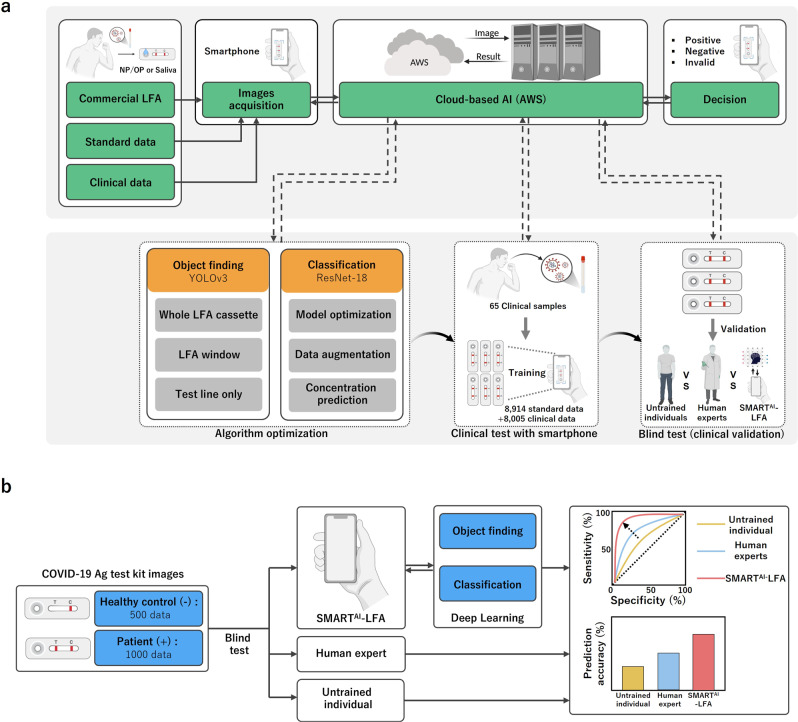
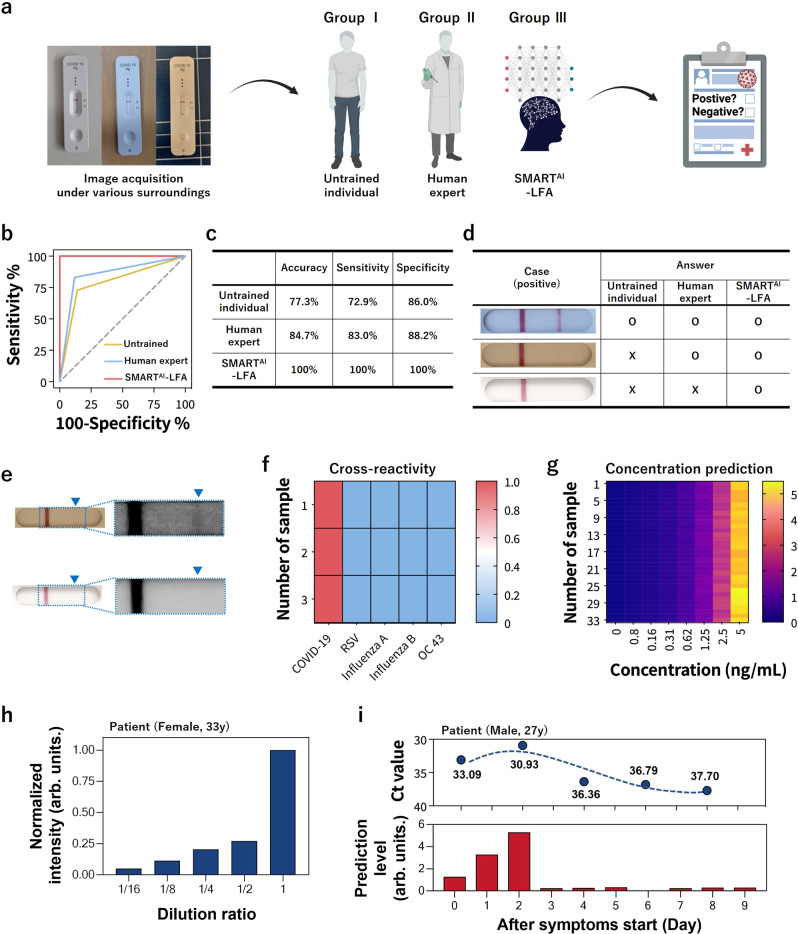
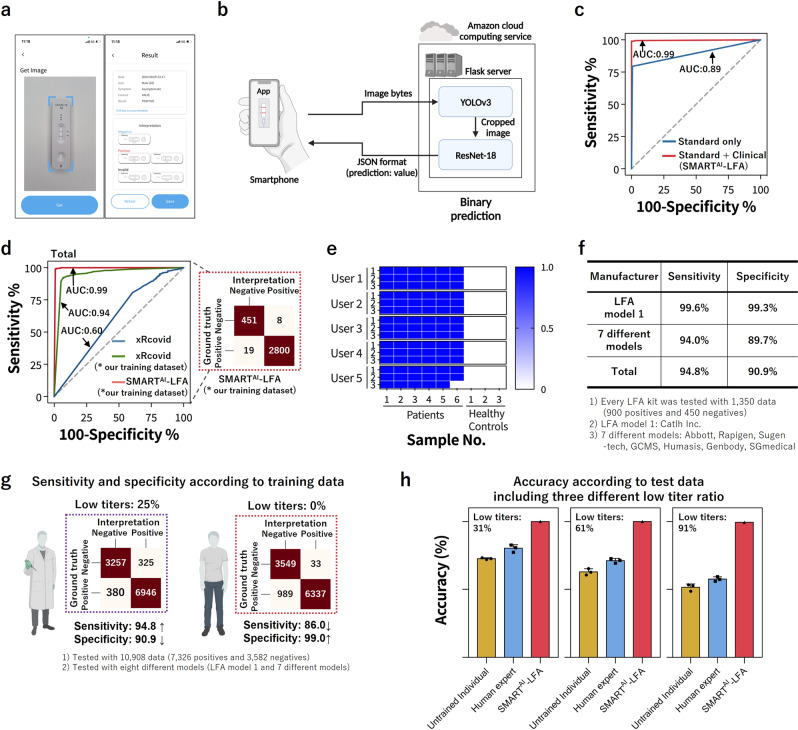
Since many lateral flow assays (LFA) are tested daily, the improvement in accuracy can greatly impact individual patient care and public health. However, current self-testing for COVID-19 detection suffers from low accuracy, mainly due to the LFA sensitivity and reading ambiguities. Here, we present deep learning-assisted smartphone-based LFA (SMARTAI-LFA) diagnostics to provide accurate decisions with higher sensitivity. Combining clinical data learning and two-step algorithms enables a cradle-free on-site assay with higher accuracy than the untrained individuals and human experts via blind tests of clinical data (n = 1500). We acquired 98% accuracy across 135 smartphone application-based clinical tests with different users/smartphones. Furthermore, with more low-titer tests, we observed that the accuracy of SMARTAI-LFA was maintained at over 99% while there was a significant decrease in human accuracy, indicating the reliable performance of SMARTAI-LFA. We envision a smartphone-based SMARTAI-LFA that allows continuously enhanced performance by adding clinical tests and satisfies the new criterion for digitalized real-time diagnostics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
