

Abolition of sagittal T7-T10 dynamics during forced ventilation in AIS patients with Lenke 1A curves
- PMID: 37095169
- PMCID: PMC10126165
- DOI: 10.1038/s41598-023-33445-z
Abolition of sagittal T7-T10 dynamics during forced ventilation in AIS patients with Lenke 1A curves
Abstract
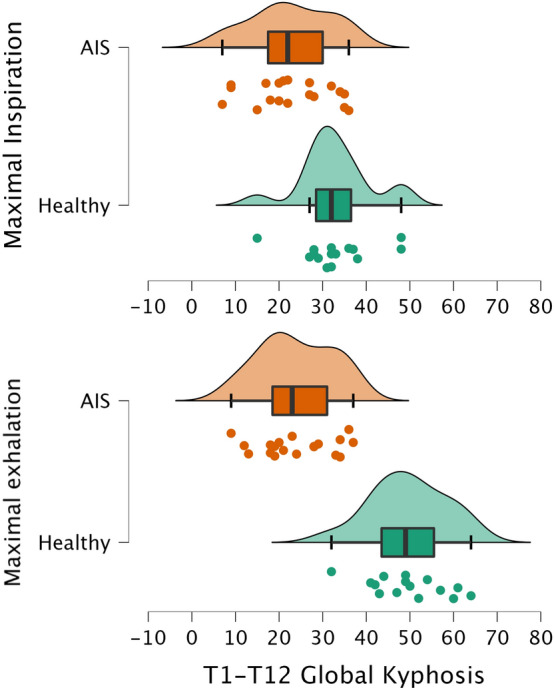
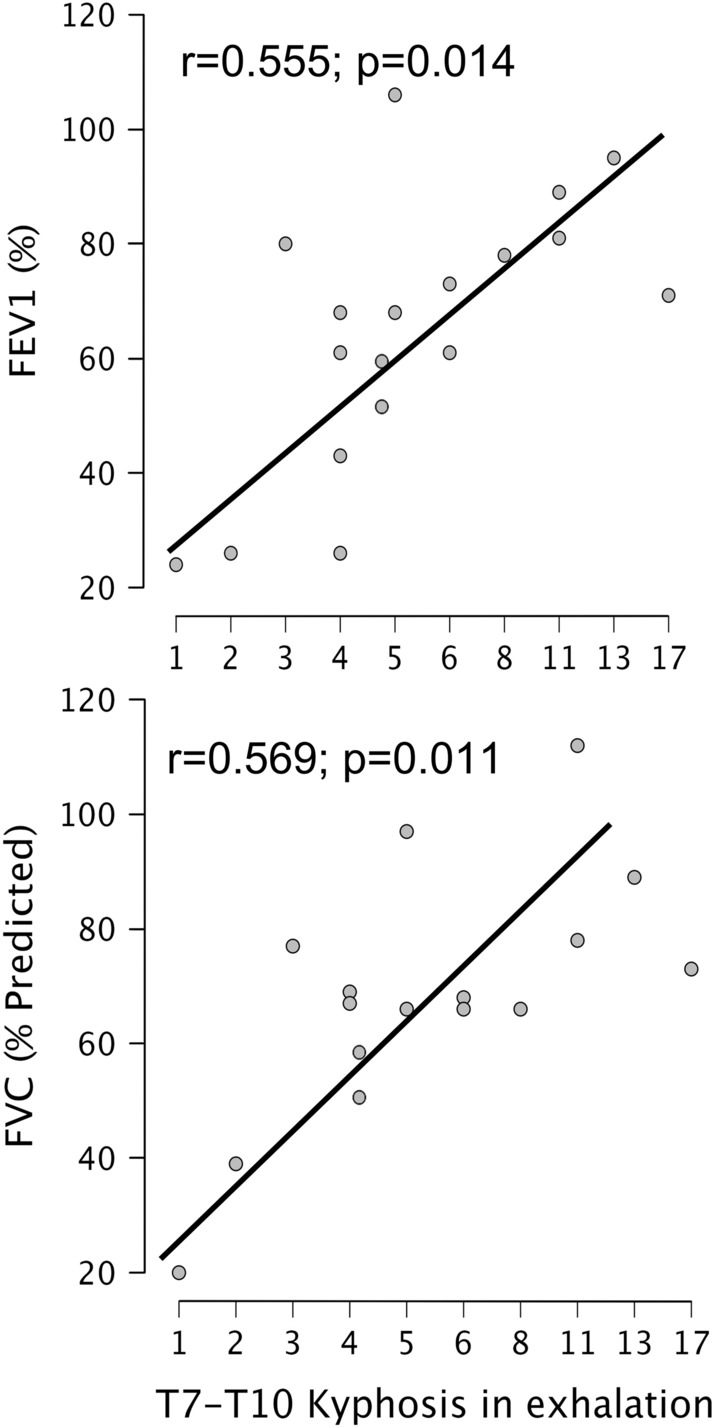
In healthy subjects, respiratory maximal volumes are highly dependent on the sagittal range of motion of the T7-T10 segment. In AIS, the abolition of T7-T10 dynamics related to the stiffness induced by the apex region in Lenke IA curves could harm ventilation during maximal breathing. The aim of this study was to analyze the dynamics of the thoracic spine during deep breathing in AIS patients and in healthy matched controls. This is a cross-sectional, case-control study. 20 AIS patients (18 girls, Cobb angle, 54.7 ± 7.9°; Risser 1.35 ± 1.2) and 15 healthy volunteers (11 girls) matched in age (12.5 versus 15.8 years mean age) were included. In AIS curves, the apex was located at T8 (14) and T9 (6). Conventional sagittal radiographs of the whole spine were performed at maximal inspiration and exhalation. The ROM of each spinal thoracic functional segment (T1-T7, T7-T10, T10-T12) and the global T1-T12 ROM were measured. In healthy subjects, the mean T1-T12 ROM during forced breathing was 16.7 ± 3.8. AIS patients showed a T1-T12 ROM of 1.1 ± 1.5 (p < 0.05), indicating a sagittal stiffness of the thoracic spine. A wide T7-T10 ROM (15.3 ± 3.0) was found in healthy controls (91.6% of the T1-T12 ROM). AIS patients showed only 0.4 ± 1.4 ROM at T7-T10 (36.4% of the T1-T12 ROM) (p < 0.001). There was a linear relationship between the magnitude of T7-T10 kyphosis in maximal exhalation and both FVC (% of predicted FVC) and FEV1. In conclusion, Lenke 1A AIS patients show a restriction of the thoracic spine motion with an almost complete abolition of T7-T10 ROM, a crucial segment for deep breathing. T7-T10 stiffness could explain the ventilatory limitations found in AIS patients.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Non-uniform Segmental Range of Motion of the Thoracic Spine During Maximal Inspiration and Exhalation in Healthy Subjects.Front Med (Lausanne). 2021 Aug 30;8:699357. doi: 10.3389/fmed.2021.699357. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34527680 Free PMC article.
-
T9 versus T10 as the upper instrumented vertebra for correction of adult deformity-rationale and recommendations.Spine J. 2017 May;17(5):615-621. doi: 10.1016/j.spinee.2016.11.008. Epub 2016 Nov 14. Spine J. 2017. PMID: 27856380
-
Flexibility assessment of the unfused thoracic segments above the "potential upper instrumented vertebrae" using the supine side bending radiographs in Lenke 5 and 6 curves for adolescent idiopathic scoliosis patients.Spine J. 2018 Jan;18(1):53-62. doi: 10.1016/j.spinee.2017.06.020. Epub 2017 Jul 24. Spine J. 2018. PMID: 28751241
-
Selective Thoracic Fusion of Lenke I and II Curves Affects Sagittal Profiles But Not Sagittal or Spinopelvic Alignment: A Case-Control Study.Spine (Phila Pa 1976). 2015 Jun 15;40(12):926-34. doi: 10.1097/BRS.0000000000000861. Spine (Phila Pa 1976). 2015. PMID: 26067149 Review.
-
Preoperative Sagittal Spinal Profile of Adolescent Idiopathic Scoliosis Lenke Types and Non-Scoliotic Adolescents: A Systematic Review and Meta-Analysis.Spine (Phila Pa 1976). 2019 Jan 15;44(2):134-142. doi: 10.1097/BRS.0000000000002748. Spine (Phila Pa 1976). 2019. PMID: 29927859
Cited by
-
Answer to the Letter to the Editor of Z. Guo, et al. concerning "Pulmonary function does not improve after 10 years of posterior spinal fusion in adolescent idiopathic scoliosis: a systematic review and meta-analysis" by Burgos J, et al. (Eur Spine J [2025]: doi: 10.1007/s00586-025-08831-y).Eur Spine J. 2025 Aug;34(8):3612-3619. doi: 10.1007/s00586-025-08992-w. Epub 2025 Jun 5. Eur Spine J. 2025. PMID: 40473971 No abstract available.
-
Pulmonary function does not improve after 10 years of posterior spinal fusion in adolescent idiopathic scoliosis: a systematic review and meta-analysis.Eur Spine J. 2025 May;34(5):1849-1860. doi: 10.1007/s00586-025-08831-y. Epub 2025 Apr 5. Eur Spine J. 2025. PMID: 40186695
-
Reply to Lemans et al. Comment on "Burgos et al. Fusionless All-Pedicle Screws for Posterior Deformity Correction in AIS Immature Patients Permit the Restoration of Normal Vertebral Morphology and Removal of the Instrumentation Once Bone Maturity Is Reached. J. Clin. Med. 2023, 12, 2408".J Clin Med. 2023 Jul 19;12(14):4773. doi: 10.3390/jcm12144773. J Clin Med. 2023. PMID: 37510888 Free PMC article.
References
-
- Newton, P.O., et al. Surgical treatment of Lenke 1 main thoracic idiopathic scoliosis: results of a prospective, multicenter study. Spine. (Phila Pa 1976)38, 328–38 (2013). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
