

Impact of age and comorbidities on SARS-CoV-2 vaccine-induced T cell immunity
- PMID: 37095240
- PMCID: PMC10124939
- DOI: 10.1038/s43856-023-00277-x
Impact of age and comorbidities on SARS-CoV-2 vaccine-induced T cell immunity
Abstract
Background: Older age and chronic disease are important risk factors for developing severe COVID-19. At population level, vaccine-induced immunity substantially reduces the risk of severe COVID-19 disease and hospitalization. However, the relative impact of humoral and cellular immunity on protection from breakthrough infection and severe disease is not fully understood.
Methods: In a study cohort of 655 primarily older study participants (median of 63 years (IQR: 51-72)), we determined serum levels of Spike IgG antibodies using a Multiantigen Serological Assay and quantified the frequency of SARS-CoV-2 Spike-specific CD4 + and CD8 + T cells using activation induced marker assay. This enabled characterization of suboptimal vaccine-induced cellular immunity. The risk factors of being a cellular hypo responder were assessed using logistic regression. Further follow-up of study participants allowed for an evaluation of the impact of T cell immunity on breakthrough infections.
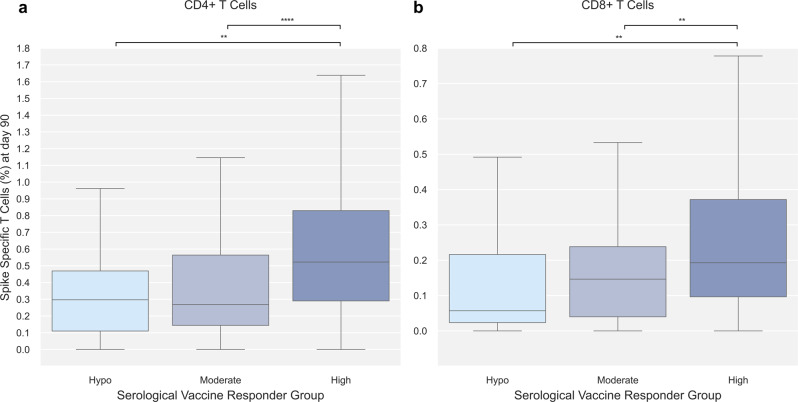
Results: We show reduced serological immunity and frequency of CD4 + Spike-specific T cells in the oldest age group (≥75 years) and higher Charlson Comorbidity Index (CCI) categories. Male sex, age group ≥75 years, and CCI > 0 is associated with an increased likelihood of being a cellular hypo-responder while vaccine type is a significant risk factor. Assessing breakthrough infections, no protective effect of T cell immunity is identified.
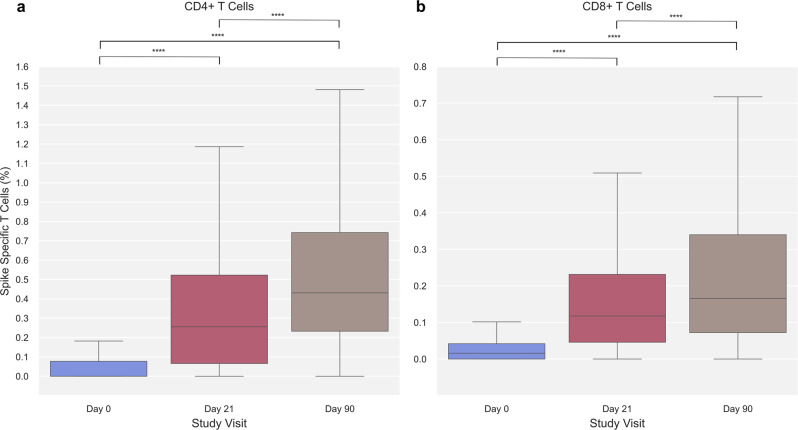
Conclusions: SARS-CoV-2 Spike-specific immune responses in both the cellular and serological compartment of the adaptive immune system increase with each vaccine dose and are progressively lower with older age and higher prevalence of comorbidities. The findings contribute to the understanding of the vaccine response in individuals with increased risk of severe COVID-19 disease and hospitalization.
Plain language summary
Vaccination has proven very effective in protecting against severe disease and hospitalization of people with COVID-19, the disease caused by SARS-CoV-2. It is still unclear, however, how the different components of the immune system respond to SARS-CoV-2 vaccination and protect from infection and severe disease. Two of the most predominant components of the immune system are specialized proteins and cells. The proteins circulate in the blood and help clear the virus by binding to it, while the cells either kill the virus or help other cells to produce more antibodies. Here, we examined the response of these two components to the SARS-CoV-2 vaccine in 655 Danish citizens. The response of both components was lower in people over 75 years old and with other diseases. These findings help in understanding the immune responses following SARS-CoV-2 vaccination in people at increased risk of severe symptoms of COVID-19.
© 2023. The Author(s).
Conflict of interest statement
NBS served as principal investigator in clinical studies from Pfizer and Gilead. All other authors declare no competing interests.
Figures



References
-
- Emborg, H.-D. et al. Vaccine effectiveness of the BNT162b2 mRNA COVID-19 vaccine against RT-PCR confirmed SARS-CoV-2 infections, hospitalisations and mortality in prioritised risk groups. medRxiv10.1101/2021.05.27.21257583 (2021).
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
