

Penehyclidine hydrochloride for treating postoperative nausea and vomiting after laparoscopic bariatric surgery: a double-blinded randomized controlled trial
- PMID: 37095439
- PMCID: PMC10124062
- DOI: 10.1186/s12871-023-02078-0
Penehyclidine hydrochloride for treating postoperative nausea and vomiting after laparoscopic bariatric surgery: a double-blinded randomized controlled trial
Abstract
Background: Postoperative nausea and vomiting (PONV) is a common and distressing complication of laparoscopic bariatric surgery (LBS). Penehyclidine hydrochloride has been reported to be effective in preventing PONV. Considering the potential preventive effects of penehyclidine against PONV, we hypothesized that intravenous infusion of penehyclidine may alleviate PONV within the first 48 h in patients scheduled for LBS.
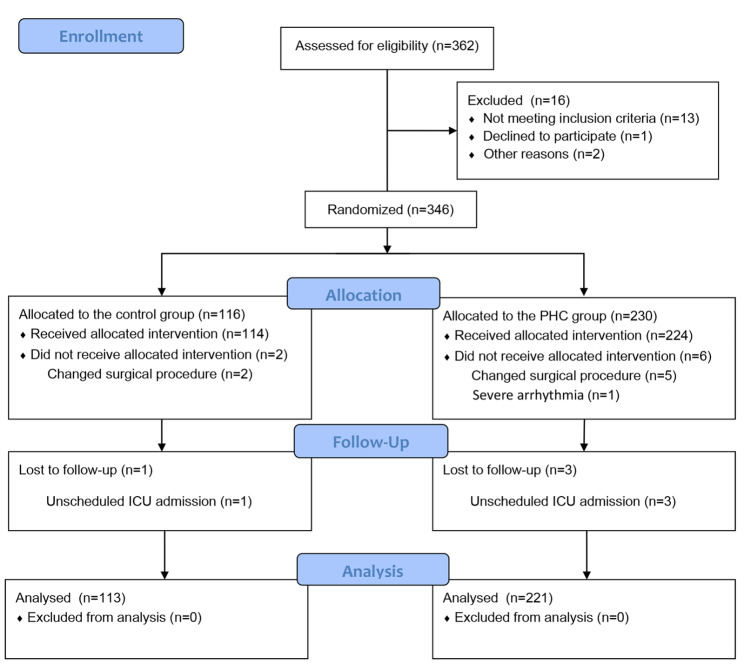
Methods: Patients who underwent LBS were randomly assigned (1:2) to receive saline (Control group, n = 113) or a single intravenous dose of penehyclidine 0.5 mg (PHC group, n = 221). The primary outcome was incidence of PONV within the first 48 h postoperatively. Secondary endpoints included severity of PONV, need for rescue antiemetic therapy, volume of water intake, and time to first flatus.
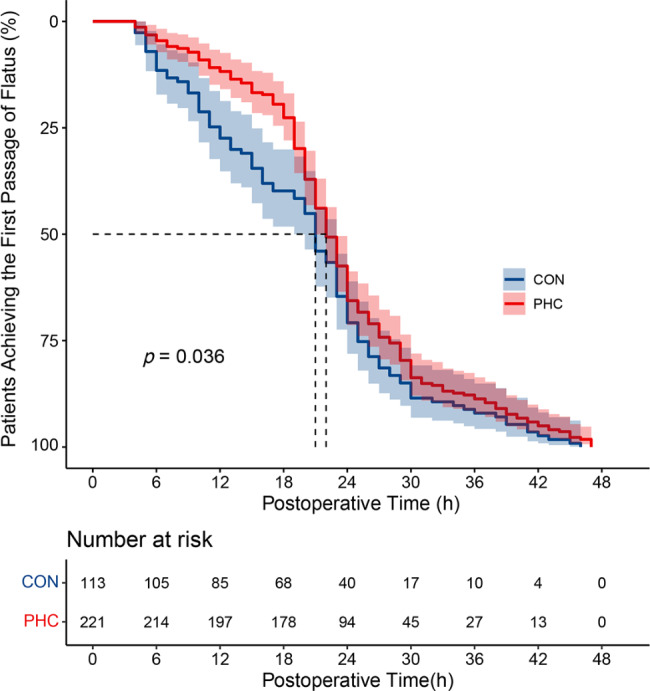
Results: PONV occurred in 159 (48%) patients within the first 48 h postoperatively, including 51% in the Control group and 46% in the PHC group. There was no significant difference in the incidence or severity of PONV between the two groups (P > 0.05). Within the first 24 h and 24-48 h, no significant difference was found in incidence or severity of PONV, postoperative nausea, postoperative vomiting, need for rescue antiemetic therapy, or volume of water intake (P > 0.05). Kaplan-Meier curves showed that penehyclidine was significantly associated with a prolonged time to first flatus (median onset time: 22 h vs. 21 h, P = 0.036).
Conclusions: Penehyclidine did not decrease incidence and severity of PONV in patients undergoing LBS. However, a single intravenous dose of penehyclidine (0.5 mg) was associated with a slightly prolonged time to first flatus.
Trial registration: Chinese Clinical Trial Registry (ChiCTR2100052418, http://www.chictr.org.cn/showprojen.aspx?proj=134893 , date of registration: 25/10/2021).
Keywords: Laparoscopic bariatric surgery; Penehyclidine hydrochloride; Postoperative nausea and vomiting; Time to first flatus.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Study of penehyclidine for the prevention of postoperative nausea and vomiting following laparoscopic sleeve gastrectomy under general anesthesia: a randomized, prospective, double-blind trial.J Anesth. 2025 Feb;39(1):67-74. doi: 10.1007/s00540-024-03424-3. Epub 2024 Nov 11. J Anesth. 2025. PMID: 39528821 Clinical Trial.
-
Use of sugammadex is associated with reduced incidence and severity of postoperative nausea and vomiting in adult patients with obesity undergoing laparoscopic bariatric surgery: a post-hoc analysis.BMC Anesthesiol. 2023 May 15;23(1):163. doi: 10.1186/s12871-023-02123-y. BMC Anesthesiol. 2023. PMID: 37189069 Free PMC article. Clinical Trial.
-
Evaluation of penehyclidine for prevention of post operative nausea and vomitting in patients undergoing total thyroidectomy under total intravenous anaesthesia with propofol-remifentanil.BMC Anesthesiol. 2022 Oct 14;22(1):317. doi: 10.1186/s12871-022-01857-5. BMC Anesthesiol. 2022. PMID: 36241968 Free PMC article. Clinical Trial.
-
Efficacy of dexmedetomidine in postoperative nausea and vomiting in laparoscopic bariatric surgery: A systematic review and meta-analysis of randomised clinical trials.Med J Malaysia. 2024 Sep;79(5):626-645. Med J Malaysia. 2024. PMID: 39352167
-
Effect of herbal medicine on postoperative nausea and vomiting after laparoscopic surgery: A systematic review and meta-analysis.Medicine (Baltimore). 2024 Jun 7;103(23):e38334. doi: 10.1097/MD.0000000000038334. Medicine (Baltimore). 2024. PMID: 38847692 Free PMC article.
Cited by
-
Penehyclidine for Prevention of Postoperative Nausea and Vomiting in Patients Undergoing Gynecological Laparoscopic Surgery Under Combined Intravenous and Inhalation Anesthesia: A Randomized, Double-Blind, Placebo-Controlled Trial.Drug Des Devel Ther. 2024 Mar 1;18:685-697. doi: 10.2147/DDDT.S453327. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 38445065 Free PMC article. Clinical Trial.
-
Postoperative Nausea and Vomiting in Female Patients Undergoing Laparoscopic Gastrointestinal Surgery with Double Prophylactic Therapy.Surg J (N Y). 2024 Jun 3;10(2):e25-e30. doi: 10.1055/s-0044-1787305. eCollection 2024 Apr. Surg J (N Y). 2024. PMID: 38835494 Free PMC article.
-
Study of penehyclidine for the prevention of postoperative nausea and vomiting following laparoscopic sleeve gastrectomy under general anesthesia: a randomized, prospective, double-blind trial.J Anesth. 2025 Feb;39(1):67-74. doi: 10.1007/s00540-024-03424-3. Epub 2024 Nov 11. J Anesth. 2025. PMID: 39528821 Clinical Trial.
-
Penehyclidine combined with antiemetics for preventing postoperative nausea and vomiting: A meta-analysis of randomized control trials and trial sequential analysis.Medicine (Baltimore). 2025 Jun 20;104(25):e42908. doi: 10.1097/MD.0000000000042908. Medicine (Baltimore). 2025. PMID: 40550034 Free PMC article.
-
Efficacy of Erector Spinae Plane Block on Analgesic Outcomes in Patients Undergoing Metabolic Surgery: A Meta-Analysis of Randomized Controlled Trials.Obes Surg. 2025 Mar;35(3):1135-1145. doi: 10.1007/s11695-025-07724-9. Epub 2025 Jan 31. Obes Surg. 2025. PMID: 39888542
References
-
- Zhu J, Wu L, Chen G, Zhao X, Chen W, Dong Z, et al. Preoperative reflux or regurgitation symptoms are independent predictors of postoperative nausea and vomiting (PONV) in patients undergoing bariatric surgery: a propensity score matching analysis. Obes Surg. 2022;32(3):819–28. doi: 10.1007/s11695-021-05859-z. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
