

The rationale and study design of two phase II trials examining the effects of BI 685,509, a soluble guanylyl cyclase activator, on clinically significant portal hypertension in patients with compensated cirrhosis
- PMID: 37095557
- PMCID: PMC10123479
- DOI: 10.1186/s13063-023-07291-3
The rationale and study design of two phase II trials examining the effects of BI 685,509, a soluble guanylyl cyclase activator, on clinically significant portal hypertension in patients with compensated cirrhosis
Abstract
Background: Clinically significant portal hypertension (CSPH) drives cirrhosis-related complications (i.e. hepatic decompensation). Impaired nitric oxide (NO) bioavailability promotes sinusoidal vasoconstriction, which is the initial pathomechanism of CSPH development. Activation of soluble guanylyl cyclase (sGC), a key downstream effector of NO, facilitates sinusoidal vasodilation, which in turn may improve CSPH. Two phase II studies are being conducted to assess the efficacy of the NO-independent sGC activator BI 685,509 in patients with CSPH due to various cirrhosis aetiologies.
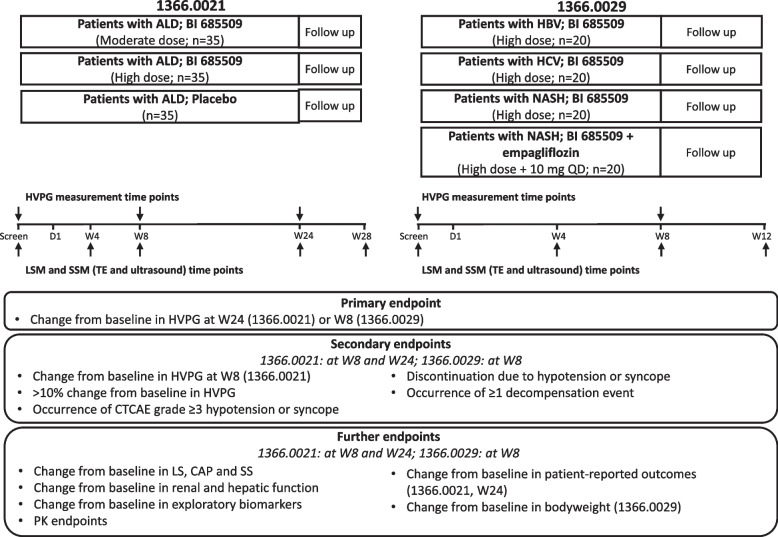
Methods: The 1366.0021 trial (NCT05161481) is a randomised, placebo-controlled, exploratory study that will assess BI 685,509 (moderate or high dose) for 24 weeks in patients with CSPH due to alcohol-related liver disease. The 1366.0029 trial (NCT05282121) is a randomised, open-label, parallel-group, exploratory study that will assess BI 685,509 (high dose) alone in patients with hepatitis B or C virus infection or non-alcoholic steatohepatitis (NASH) and in combination with 10 mg empagliflozin in patients with NASH and type 2 diabetes mellitus for 8 weeks. The 1366.0021 trial will enrol 105 patients, and the 1366.0029 trial will enrol 80 patients. In both studies, the primary endpoint is the change from baseline in hepatic venous pressure gradient (HVPG) until the end of treatment (24 or 8 weeks, respectively). Secondary endpoints include the proportion of patients with an HVPG reduction of > 10% from baseline, the development of decompensation events and the change from baseline in HVPG after 8 weeks in the 1366.0021 trial. In addition, the trials will assess changes in liver and spleen stiffness by transient elastography, changes in hepatic and renal function and the tolerability of BI 685,509.
Discussion: These trials will enable the assessment of the short-term (8 weeks) and longer-term (24 weeks) effects and safety of sGC activation by BI 685,509 on CSPH due to various cirrhosis aetiologies. The trials will use central readings of the diagnostic gold standard HVPG for the primary endpoint, as well as changes in established non-invasive biomarkers, such as liver and spleen stiffness. Ultimately, these trials will provide key information for developing future phase III trials.
Trial registration: 1366.0021: EudraCT no. 2021-001,285-38; ClinicalTrials.gov NCT05161481. Registered on 17 December 2021, https://www.
Clinicaltrials: gov/ct2/show/NCT05161481 . 1366.0029: EudraCT no. 2021-005,171-40; ClinicalTrials.gov NCT05282121. Registered on 16 March 2022, https://www.
Clinicaltrials: gov/ct2/show/NCT05282121 .
Keywords: Alcohol-related liver disease; Cirrhosis; Hepatitis B virus; Hepatitis C virus; Non-alcoholic steatohepatitis; Portal hypertension.
© 2023. The Author(s).
Conflict of interest statement
TR has received grant support from AbbVie, Boehringer Ingelheim, Gilead Sciences, Gore, Intercept Pharmaceuticals, MSD, MYR Pharmaceuticals, Philips Healthcare, Pliant and Siemens; speaking honoraria from AbbVie, Gilead Sciences, Gore, Intercept Pharmaceuticals, MSD and Roche; consulting or advisory board fees from AbbVie, Bayer, Boehringer Ingelheim, Gilead Sciences, Intercept Pharmaceuticals, MSD and Siemens; and travel support from AbbVie, Boehringer Ingelheim, Gilead Sciences and Roche. AB has been an advisory board member for Inventiva, Bracco, General Electrics, and Boehringer Ingelheim. JT has received speaking and/or consulting fees from Versantis, Gore, Boehringer-Ingelheim, Alexion, Falk, Mallinckrodt, Grifols and CSL Behring and was supported by the German Research Foundation (DFG) project ID 403224013 – SFB 1382 (A09), by the German Federal Ministry of Education and Research (BMBF) for the DEEP-HCC project and by the Hessian Ministry of Higher Education, Research and the Arts (HMWK) for the ENABLE and ACLF-I cluster projects. The MICROB-PREDICT (project ID 825694), DECISION (project ID 847949), GALAXY (project ID 668031), LIVERHOPE (project ID 731875) and IHMCSA (project ID 964590) projects have received funding from the European Union’s Horizon 2020 research and innovation programme. JE, IG, RS and AT are employees of Boehringer Ingelheim. The manuscript reflects only the authors’ views, and the European Commission is not responsible for any use that may be made of the information it contains. The funders had no influence on the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures
Similar articles
-
Randomized placebo-controlled trial of emricasan for non-alcoholic steatohepatitis-related cirrhosis with severe portal hypertension.J Hepatol. 2020 May;72(5):885-895. doi: 10.1016/j.jhep.2019.12.010. Epub 2019 Dec 21. J Hepatol. 2020. PMID: 31870950 Clinical Trial.
-
Carvedilol to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension stratified by liver stiffness: study protocol for a randomied, double-blind, placebo-controlled, multicentre trial in China.BMJ Open. 2024 Jul 11;14(7):e081623. doi: 10.1136/bmjopen-2023-081623. BMJ Open. 2024. PMID: 38991669 Free PMC article.
-
Assessment of the Performance of Non-invasive Criteria for the Evaluation of Clinically Significant Portal Hypertension in Patients with Compensated Advanced Chronic Liver Disease.Dig Dis Sci. 2023 May;68(5):2149-2157. doi: 10.1007/s10620-022-07778-0. Epub 2022 Dec 23. Dig Dis Sci. 2023. PMID: 36562888
-
Non-Invasive Diagnostic Tests for Portal Hypertension in Patients with HBV- and HCV-Related Cirrhosis: A Comprehensive Review.Medicina (Kaunas). 2024 Apr 24;60(5):690. doi: 10.3390/medicina60050690. Medicina (Kaunas). 2024. PMID: 38792873 Free PMC article. Review.
-
The Value of Liver and Spleen Stiffness for Evaluation of Portal Hypertension in Compensated Cirrhosis.Hepatol Commun. 2022 May;6(5):950-964. doi: 10.1002/hep4.1855. Epub 2021 Dec 14. Hepatol Commun. 2022. PMID: 34904404 Free PMC article. Review.
Cited by
-
Decoding signaling mechanisms: unraveling the targets of guanylate cyclase agonists in cardiovascular and digestive diseases.Front Pharmacol. 2023 Dec 20;14:1272073. doi: 10.3389/fphar.2023.1272073. eCollection 2023. Front Pharmacol. 2023. PMID: 38186653 Free PMC article. Review.
-
Hepatic immune regulation and sex disparities.Nat Rev Gastroenterol Hepatol. 2024 Dec;21(12):869-884. doi: 10.1038/s41575-024-00974-5. Epub 2024 Sep 5. Nat Rev Gastroenterol Hepatol. 2024. PMID: 39237606 Review.
-
Molecular patterns of the NO-sGC-cGMP pathway in progressive and regressive liver fibrosis models.Sci Rep. 2025 Jul 25;15(1):27051. doi: 10.1038/s41598-025-12381-0. Sci Rep. 2025. PMID: 40715433 Free PMC article.
-
Mechanisms and implications of recompensation in cirrhosis.JHEP Rep. 2024 Oct 10;6(12):101233. doi: 10.1016/j.jhepr.2024.101233. eCollection 2024 Dec. JHEP Rep. 2024. PMID: 39640222 Free PMC article. Review.
-
Recent advances in the prevention and treatment of decompensated cirrhosis and acute-on-chronic liver failure (ACLF) and the role of biomarkers.Gut. 2024 May 10;73(6):1015-1024. doi: 10.1136/gutjnl-2023-330584. Gut. 2024. PMID: 38527788 Free PMC article. Review.
References
-
- Reiberger T, Schwabl P, Trauner M, et al. Measurement of the hepatic venous pressure gradient and transjugular liver biopsy. J Vis Exp 2020(160). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
