

Surgical trial design for incorporating the effects of learning: what is the current methodological guidance, and is it sufficient?
- PMID: 37095568
- PMCID: PMC10127059
- DOI: 10.1186/s13063-023-07265-5
Surgical trial design for incorporating the effects of learning: what is the current methodological guidance, and is it sufficient?
Abstract
Background: Surgical interventions are complex. Key elements of this complexity are the surgeon and their learning curve. They pose methodological challenges in the design, analysis and interpretation of surgical RCTs. We identify, summarise, and critically examine current guidance about how to incorporate learning curves in the design and analysis of RCTs in surgery.
Examining current guidance: Current guidance presumes that randomisation must be between levels of just one treatment component, and that the evaluation of comparative effectiveness will be made via the average treatment effect (ATE). It considers how learning effects affect the ATE, and suggests solutions which seek to define the target population such that the ATE is a meaningful quantity to guide practice. We argue that these are solutions to a flawed formulation of the problem, and are inadequate for policymaking in this setting.
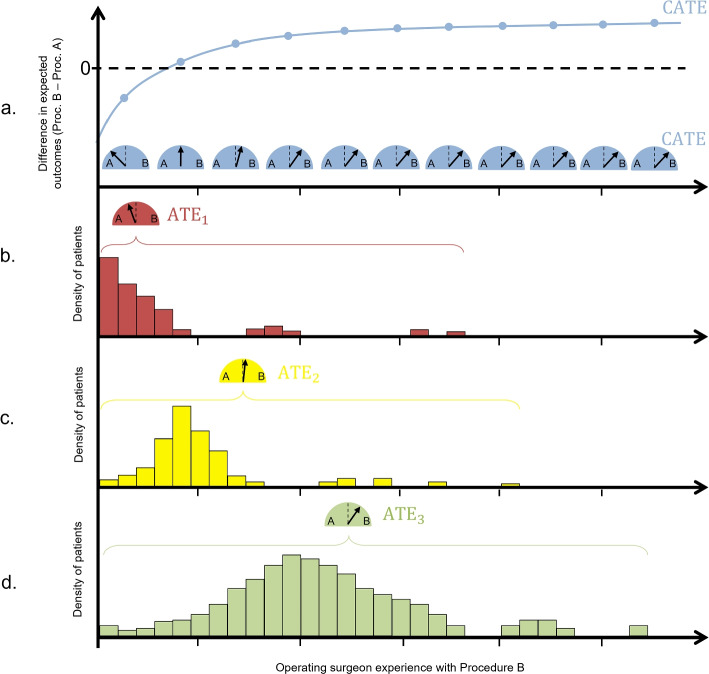
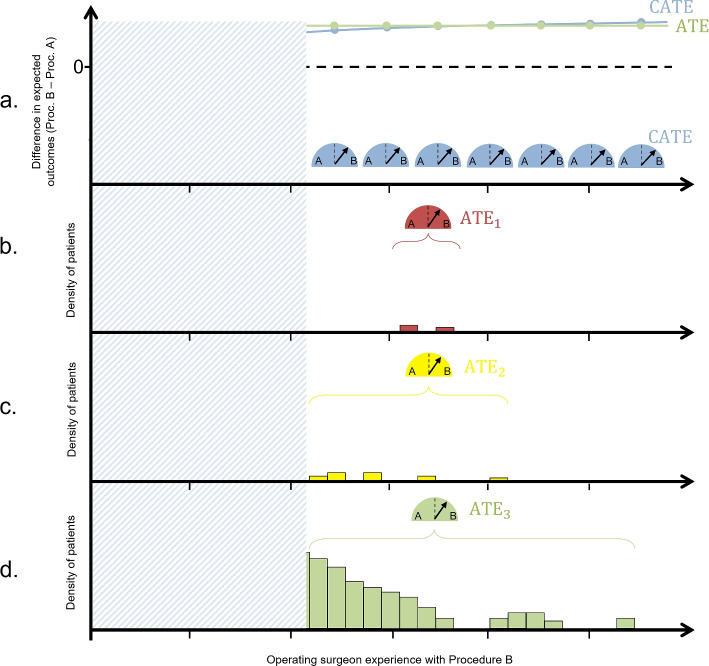
Reformulating the problem: The premise that surgical RCTs are limited to single-component comparisons, evaluated via the ATE, has skewed the methodological discussion. Forcing a multi-component intervention, such as surgery, into the framework of the conventional RCT design ignores its factorial nature. We briefly discuss the multiphase optimisation strategy (MOST), which for a Stage 3 trial would endorse a factorial design. This would provide a wealth of information to inform nuanced policy but would likely be infeasible in this setting. We discuss in more depth the benefits of targeting the ATE conditional on operating surgeon experience (CATE). The value of estimating the CATE for exploring learning effects has been previously recognised, but with discussion limited to analysis methods only. The robustness and precision of such analyses can be ensured via the trial design, and we argue that trial designs targeting CATE represent a clear gap in current guidance.
Conclusion: Trial designs that facilitate robust, precise estimation of the CATE would allow for more nuanced policymaking, leading to patient benefit. No such designs are currently forthcoming. Further research in trial design to facilitate the estimation of the CATE is needed.
Keywords: Design; Learning curve; Learning effects; Surgical RCTs; Surgical trials.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
The effectiveness of internet-based e-learning on clinician behavior and patient outcomes: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):52-64. doi: 10.11124/jbisrir-2015-1919. JBI Database System Rev Implement Rep. 2015. PMID: 26447007
-
Expertise-based design in surgical trials: a narrative review.Can J Surg. 2021 Nov 10;64(6):E594-E602. doi: 10.1503/cjs.008520. Print 2021 Nov-Dec. Can J Surg. 2021. PMID: 34759044 Free PMC article.
-
Assessment of learning curves in complex surgical interventions: a consecutive case-series study.Trials. 2016 Jun 1;17(1):266. doi: 10.1186/s13063-016-1383-4. Trials. 2016. PMID: 27245050 Free PMC article.
-
Statistical assessment of the learning curves of health technologies.Health Technol Assess. 2001;5(12):1-79. doi: 10.3310/hta5120. Health Technol Assess. 2001. PMID: 11319991 Review.
Cited by
-
Evidence-Based Medicine Within Surgical Practice and Training: A Scoping Review.World J Surg. 2025 Apr;49(4):916-929. doi: 10.1002/wjs.12479. Epub 2025 Feb 4. World J Surg. 2025. PMID: 39904742 Free PMC article.
-
Evidence-based surgical procedures to optimize caesarean outcomes: an overview of systematic reviews.EClinicalMedicine. 2024 May 19;72:102632. doi: 10.1016/j.eclinm.2024.102632. eCollection 2024 Jun. EClinicalMedicine. 2024. PMID: 38812964 Free PMC article. Review.
-
Accounting for the learning curve effect in surgical trials: Post-hoc analysis of the prophylactic use of biologic mesh in ileal conduit (PUBMIC) trial.Investig Clin Urol. 2025 May;66(3):281-283. doi: 10.4111/icu.20250030. Investig Clin Urol. 2025. PMID: 40312908 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
