

Imaging Follow-Up of Nonsurgical Therapies for Lung Cancer: AJR Expert Panel Narrative Review
- PMID: 37095669
- PMCID: PMC11037936
- DOI: 10.2214/AJR.23.29104
Imaging Follow-Up of Nonsurgical Therapies for Lung Cancer: AJR Expert Panel Narrative Review
Abstract
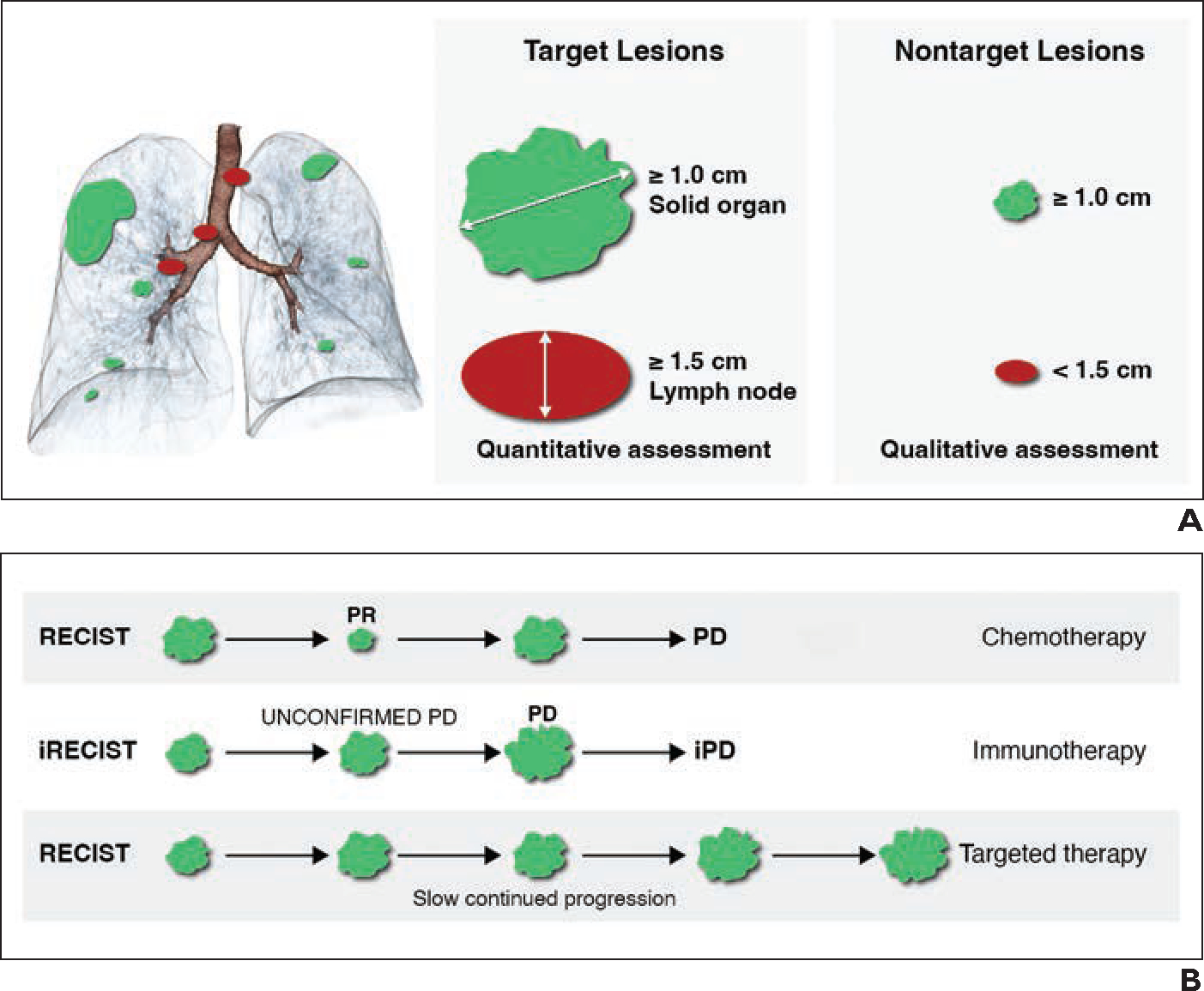
Lung cancer continues to be the most common cause of cancer-related death worldwide. In the past decade, with the implementation of lung cancer screening programs and advances in surgical and nonsurgical therapies, the survival of patients with lung cancer has increased, as has the number of imaging studies that these patients undergo. However, most patients with lung cancer do not undergo surgical re-section, because they have comorbid disease or lung cancer in an advanced stage at diagnosis. Nonsurgical therapies have continued to evolve with a growing range of systemic and targeted therapies, and there has been an associated evolution in the imaging findings encountered at follow-up examinations after such therapies (e.g., with respect to posttreatment changes, treatment complications, and recurrent tumor). This AJR Expert Panel Narrative Review describes the current status of nonsurgical therapies for lung cancer and their expected and unexpected imaging manifestations. The goal is to provide guidance to radiologists regarding imaging assessment after such therapies, focusing mainly on non-small cell lung cancer. Covered therapies include systemic therapy (conventional chemotherapy, targeted therapy, and immunotherapy), radiotherapy, and thermal ablation.
Keywords: RECIST; ablation; imaging follow-up; lung cancer; radiation therapy; response assessment; targeted therapy.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71:209–249 - PubMed
-
- Ettinger DS, Wood DE, Aisner DL, et al. Non–small cell lung cancer, version 3.2022: NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2022; 20:497–530 - PubMed
-
- American Lung Association website. State of lung cancer. www.Lung.org/solc. Published 2021. Accessed Jun 29, 2022
-
- Carter BW, Altan M, Shroff GS, Truong MT, Vlahos I. Post-chemotherapy and targeted therapy imaging of the chest in lung cancer. Clin Radiol 2022; 77:e1–e10 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
