

Endoscopically assisted selective antegrade cardioplegia in minimally invasive aortic valve replacement for patients with aortic insufficiency
- PMID: 37096103
- PMCID: PMC10122126
- DOI: 10.1016/j.xjtc.2023.01.002
Endoscopically assisted selective antegrade cardioplegia in minimally invasive aortic valve replacement for patients with aortic insufficiency
Abstract
Objective: In minimally invasive aortic valve replacement via a right minithoracotomy for patients with significant aortic insufficiency, optimal cardioplegia delivery procedures remain controversial. This study aimed to describe and evaluate endoscopically assisted selective cardioplegia delivery in minimally invasive aortic valve replacement for aortic insufficiency.
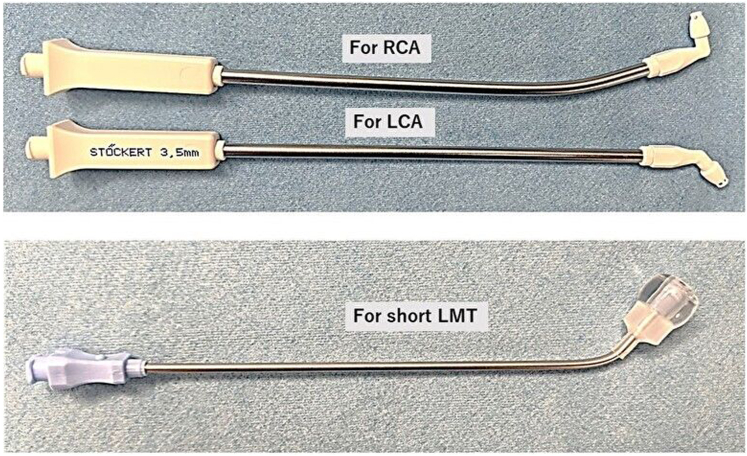
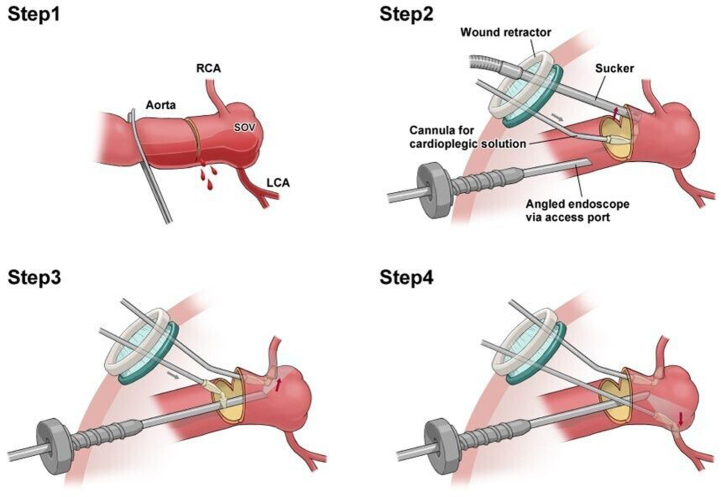
Methods: Between September 2015 and February 2022, 104 patients (mean age, 66.0 ± 14.3 years) with moderate or greater aortic insufficiency underwent endoscopically assisted minimally invasive aortic valve replacement at our institutions. For myocardial protection, potassium chloride and landiolol were systemically administered before aortic crossclamping, and cold crystalloid cardioplegia was delivered selectively to the coronary arteries using step-by-step endoscopic procedures. The early clinical outcomes were also evaluated.
Results: Eighty-four patients (80.7%) had severe aortic insufficiency, and 13 patients (12.5%) had aortic stenosis and moderate or greater aortic insufficiency. A regular prosthesis was used in 97 cases (93.3%), and a sutureless prosthesis was used in 7 cases (6.7%). The mean operative, cardiopulmonary bypass, and aortic crossclamping times were 169.3 ± 36.5, 102.4 ± 25.4, and 72.5 ± 21.8 minutes, respectively. No patients underwent a conversion to full sternotomy or required mechanical circulatory support during or after surgery. No operative deaths or perioperative myocardial infarctions occurred. The median intensive care unit and hospital stays were 1 and 5 days, respectively.
Conclusions: Endoscopically assisted selective antegrade cardioplegia delivery is safe and feasible for treating minimally invasive aortic valve replacement in patients with significant aortic insufficiency.
Keywords: aortic insufficiency; aortic valve replacement; cardioplegia; endoscopic surgery; minimally invasive cardiac surgery.
© 2023 The Author(s).
Figures




Similar articles
-
Right anterior minithoracotomy for aortic valve replacement: 10-year experience of a single center.J Thorac Cardiovasc Surg. 2015 Sep;150(3):548-56.e2. doi: 10.1016/j.jtcvs.2015.06.045. Epub 2015 Jun 29. J Thorac Cardiovasc Surg. 2015. PMID: 26215359
-
Ministernotomy aortic valve surgery in patients with prior patent mammary artery grafts after coronary artery bypass grafting.Eur J Cardiothorac Surg. 2019 Jun 1;55(6):1174-1179. doi: 10.1093/ejcts/ezy442. Eur J Cardiothorac Surg. 2019. PMID: 30649235
-
Cold blood cardioplegia reduces the increase in cardiac enzyme levels compared with cold crystalloid cardioplegia in patients undergoing aortic valve replacement for isolated aortic stenosis.J Thorac Cardiovasc Surg. 2010 Apr;139(4):874-80. doi: 10.1016/j.jtcvs.2009.05.036. Epub 2009 Jul 26. J Thorac Cardiovasc Surg. 2010. PMID: 19660338 Clinical Trial.
-
Should minimally invasive aortic valve replacement be restricted to primary interventions?Thorac Cardiovasc Surg. 2007 Aug;55(5):304-9. doi: 10.1055/s-2007-965283. Thorac Cardiovasc Surg. 2007. PMID: 17629860
-
Minimal access versus conventional aortic valve replacement: a meta-analysis of propensity-matched studies.Interact Cardiovasc Thorac Surg. 2017 Oct 1;25(4):624-632. doi: 10.1093/icvts/ivx212. Interact Cardiovasc Thorac Surg. 2017. PMID: 28962507 Review.
Cited by
-
Aortic valve replacement through right anterior mini-thoracotomy in patients with chronic severe aortic regurgitation: a retrospective single-center study.J Yeungnam Med Sci. 2024 Jul;41(3):213-219. doi: 10.12701/jyms.2024.00290. Epub 2024 Jun 12. J Yeungnam Med Sci. 2024. PMID: 38863223 Free PMC article.
References
-
- Glauber M., Miceli A., Bevilacqua S., Farneti P.A. Minimally invasive aortic valve replacement via right anterior minithoracotomy: early outcomes and midterm follow-up. J Thorac Cardiovasc Surg. 2011;142:1577–1579. - PubMed
-
- Tabata M., Umakanthan R., Khalpey Z., Aranki S.F., Couper G.S., Shekar P.S., et al. Conversion to full sternotomy during minimal-access cardiac surgery: reasons and results during a 9.5-year experience. J Thorac Cardiovasc Surg. 2007;134:165–169. - PubMed
-
- Panos A.L., Ali I.S., Birnbaum P.L., Barrozo C.A., al-Nowaiser O., Salerno T.A. Coronary sinus injuries during retrograde continuous normothermic blood cardioplegia. Ann Thorac Surg. 1992;54:1137–1138. - PubMed
LinkOut - more resources
Full Text Sources
