

Palbociclib Adherence and Persistence in Patients with Hormone Receptor Positive/Human Epidermal Growth Factor Receptor 2 Negative (HR+/HER2-) Metastatic Breast Cancer
- PMID: 37096162
- PMCID: PMC10122484
- DOI: 10.2147/PPA.S401480
Palbociclib Adherence and Persistence in Patients with Hormone Receptor Positive/Human Epidermal Growth Factor Receptor 2 Negative (HR+/HER2-) Metastatic Breast Cancer
Abstract
Purpose: To assess adherence and persistence with palbociclib therapy in patients with HR+/HER2- metastatic breast cancer (mBC) in a US real-world setting.
Methods: This retrospective study evaluated palbociclib dosing, adherence, and persistence using commercial and Medicare Advantage with Part D claims data from the Optum Research Database. Adult patients with mBC who had continuous enrollment 12 months prior to mBC diagnosis and initiated first-line palbociclib with aromatase inhibitor (AI) or fulvestrant between 02/03/2015 and 12/31/2019 were included. Demographic and clinical characteristics, palbociclib dosing and dose changes, adherence (medication possession ratio [MPR]), and persistence were measured. Adjusted logistic and Cox regression models were used to examine demographic and clinical factors associated with adherence and discontinuation.
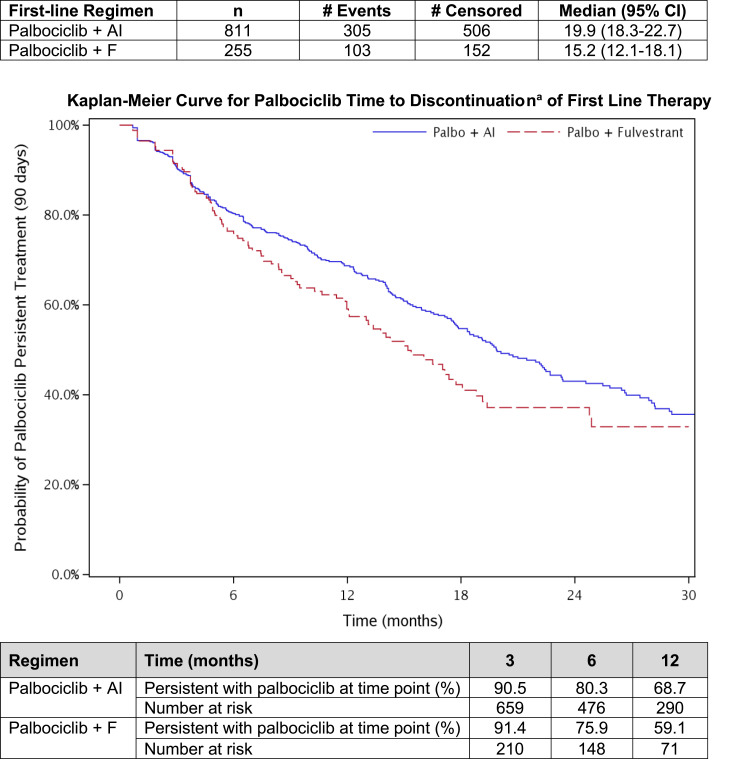
Results: Patients (n = 1066) with a mean age of 66 years were included; 76.1% received first-line palbociclib+AI and 23.9% palbociclib+fulvestrant. Most patients (85.7%) initiated palbociclib at 125 mg/day. Of the 34.0% of patients with a dose reduction, 82.6% reduced from 125 to 100 mg/day. Overall, 80.0% of patients were adherent (MPR), and 38.3% discontinued palbociclib during a mean (SD) follow-up of 16.0 (11.2) and 17.4 (13.4) months, for palbociclib+fulvestrant and palbociclib+AI, respectively. Annual income below $75,000 was significantly associated with poor adherence. Older age (age 65-74 years (hazard ratio [HR] 1.57, 95% CI, 1.06, 2.33), age ≥75 years (HR 1.61, 95% CI: 1.08, 2.41)) and bone-only metastatic disease (HR 1.37, 95% CI, 1.06, 1.76) were significantly associated with palbociclib discontinuation.
Conclusion: In this real-world study, >85% of patients started palbociclib at 125 mg/day and 1 in 3 had dose reductions during the follow-up. Patients were generally adherent and persistent with palbociclib. Older age, bone-only disease, and low-income levels were associated with early discontinuation or non-adherence. Further studies are needed to understand the associations of clinical and economic outcomes with palbociclib adherence and persistence.
Keywords: adherence; breast cancer; metastatic; palbociclib; persistence.
© 2023 Engel-Nitz et al.
Conflict of interest statement
Ashley S. Cha-Silva, Samantha K. Kurosky and Xianchen Liu, are employees of and hold stock in Pfizer. Nicole M. Engel-Nitz, Mary G. Johnson and Michael P. Johnson are employees of Optum, which was contracted by Pfizer to conduct this study, and hold stock in UnitedHealth Group. The authors report no other conflicts of interest in this work.
Figures




Similar articles
-
Treatment patterns and clinical outcomes among patients receiving palbociclib in combination with an aromatase inhibitor or fulvestrant for HR+/HER2-negative advanced/metastatic breast cancer in real-world settings in the US: Results from the IRIS study.Breast. 2019 Feb;43:22-27. doi: 10.1016/j.breast.2018.10.009. Epub 2018 Oct 20. Breast. 2019. PMID: 30391832
-
Real-World Tumor Response of Palbociclib in Combination With an Aromatase Inhibitor as First-Line Therapy in Pre/Perimenopausal Women With Metastatic Breast Cancer.Target Oncol. 2023 Jul;18(4):543-558. doi: 10.1007/s11523-023-00979-1. Epub 2023 Jul 10. Target Oncol. 2023. PMID: 37428347 Free PMC article.
-
Real-world treatment patterns and effectiveness of palbociclib plus an aromatase inhibitor in patients with metastatic breast cancer aged 75 years or older.Front Oncol. 2023 Sep 28;13:1237751. doi: 10.3389/fonc.2023.1237751. eCollection 2023. Front Oncol. 2023. PMID: 37841423 Free PMC article.
-
Palbociclib: A Novel Cyclin-Dependent Kinase Inhibitor for Hormone Receptor-Positive Advanced Breast Cancer.Ann Pharmacother. 2015 Nov;49(11):1252-60. doi: 10.1177/1060028015602273. Epub 2015 Aug 31. Ann Pharmacother. 2015. PMID: 26324355 Free PMC article. Review.
-
Palbociclib: A New Option for Front-Line Treatment of Metastatic, Hormone Receptor-Positive, HER2-Negative Breast Cancer.J Adv Pract Oncol. 2015 Nov-Dec;6(6):577-81. Epub 2015 Nov 1. J Adv Pract Oncol. 2015. PMID: 27648347 Free PMC article. Review. No abstract available.
Cited by
-
Palbociclib in Older Patients with Advanced/Metastatic Breast Cancer: A Systematic Review.Target Oncol. 2024 May;19(3):303-320. doi: 10.1007/s11523-024-01046-z. Epub 2024 Mar 28. Target Oncol. 2024. PMID: 38546943 Free PMC article.
-
Real-World Efficacy and Adherence to Palbociclib in HR-Positive, HER2-Negative Advanced Breast Cancer: Insights from a Romanian Cohort.Cancers (Basel). 2024 Dec 13;16(24):4161. doi: 10.3390/cancers16244161. Cancers (Basel). 2024. PMID: 39766060 Free PMC article.
-
Non-adherence of cyclin-dependent kinases 4 and 6 inhibitors reduces overall and progression-free survival in patients with hormone receptor-positive breast cancer.Breast Cancer Res Treat. 2025 Jul;212(1):71-78. doi: 10.1007/s10549-025-07701-x. Epub 2025 Apr 16. Breast Cancer Res Treat. 2025. PMID: 40237878
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer v8.2021; 2021. Available from: https://www.nccn.org/professionals/physician_gls/pdf/breast_blocks.pdf. Accessed November 11, 2021.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
