

Identification of Adult Patients With Classical Dyskeratosis Congenita or Cryptic Telomere Biology Disorder by Telomere Length Screening Using Age-modified Criteria
- PMID: 37096215
- PMCID: PMC10121438
- DOI: 10.1097/HS9.0000000000000874
Identification of Adult Patients With Classical Dyskeratosis Congenita or Cryptic Telomere Biology Disorder by Telomere Length Screening Using Age-modified Criteria
Abstract
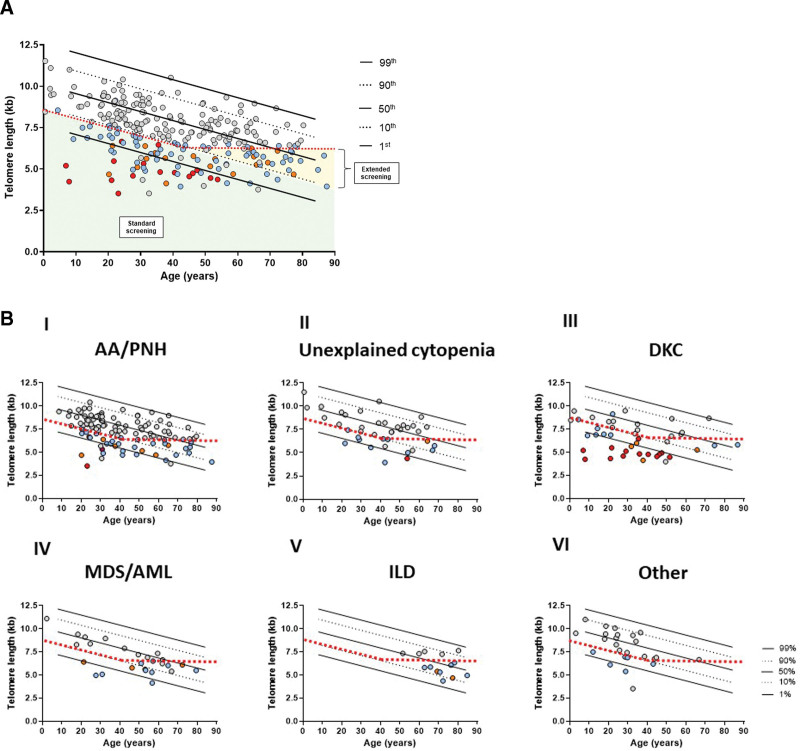
Telomere biology disorders (TBD) result from premature telomere shortening due to pathogenic germline variants in telomere maintenance-associated genes. In adults, TBD are characterized by mono/oligosymptomatic clinical manifestations (cryptic TBD) contributing to severe underdiagnosis. We present a prospective multi-institutional cohort study where telomere length (TL) screening was performed in either newly diagnosed patients with aplastic anemia (AA) or if TBD was clinically suspected by the treating physician. TL of 262 samples was measured via flow-fluorescence in situ hybridization (FISH). TL was considered suspicious once below the 10th percentile of normal individuals (standard screening) or if below 6.5 kb in patients >40 years (extended screening). In cases with shortened TL, next generation sequencing (NGS) for TBD-associated genes was performed. The patients referred fell into 6 different screening categories: (1) AA/paroxysmal nocturnal hemoglobinuria, (2) unexplained cytopenia, (3) dyskeratosis congenita, (4) myelodysplastic syndrome/acute myeloid leukemia, (5) interstitial lung disease, and (6) others. Overall, TL was found to be shortened in 120 patients (n = 86 standard and n = 34 extended screening). In 17 of the 76 (22.4%) standard patients with sufficient material for NGS, a pathogenic/likely pathogenic TBD-associated gene variant was identified. Variants of uncertain significance were detected in 17 of 76 (22.4%) standard and 6 of 29 (20.7%) extended screened patients. Expectedly, mutations were mainly found in TERT and TERC. In conclusion, TL measured by flow-FISH represents a powerful functional in vivo screening for an underlying TBD and should be performed in every newly diagnosed patient with AA as well as other patients with clinical suspicion for an underlying TBD in both children and adults.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Conflict of interest statement
THB and FB have a long-ranging scientific collaboration with Repeat Dx., Vancouver, Canada. All the other authors have no conflicts of interest to disclose.
Figures



References
-
- Martinez P, Blasco MA. Telomeric and extra-telomeric roles for telomerase and the telomere-binding proteins. Nat Rev Cancer. 2011;11:161–176. - PubMed
-
- Tummala H, Walne A, Dokal I. The biology and management of dyskeratosis congenita and related disorders of telomeres. Expert Rev Hematol. 2022;15:685–696. - PubMed
LinkOut - more resources
Full Text Sources