

Burden of idiopathic inflammatory rheumatic diseases in occupational healthcare: increased absenteeism and healthcare resource utilization
- PMID: 37096788
- PMCID: PMC10713983
- DOI: 10.5271/sjweh.4095
Burden of idiopathic inflammatory rheumatic diseases in occupational healthcare: increased absenteeism and healthcare resource utilization
Abstract
Objectives: Patients with idiopathic inflammatory rheumatic diseases (IIRD) often have decreased working capacity resulting in indirect costs. However, data on patients' short-term sick leave has been limited. This retrospective cohort study evaluated the number and length of sick leave, including short-term leave, and occupational healthcare resource utilization (HCRU) of the working-aged patients with IIRD compared to controls.
Methods: The data on sick leave and occupational HCRU were gathered from the electronic medical records of the largest occupational healthcare provider in Finland from January 2012 to December 2019. Employed patients with an IIRD (including rheumatoid arthritis, spondyloarthritis, psoriatic and enteropathic arthritis, juvenile arthritis, and reactive arthritis) with at least a 12-months follow-up were identified and compared to age-, sex-, and follow-up matched controls without IIRD.
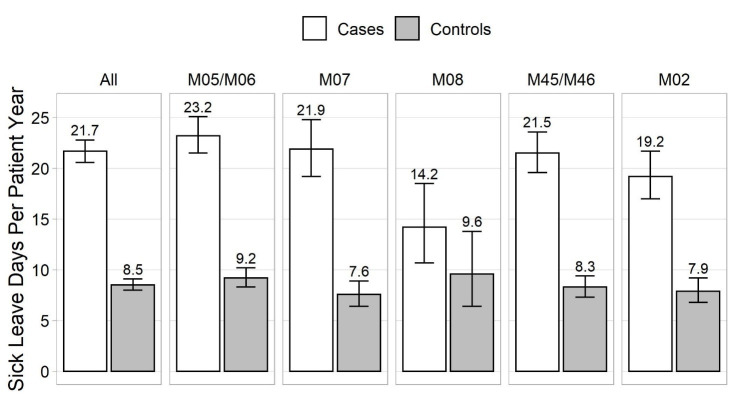
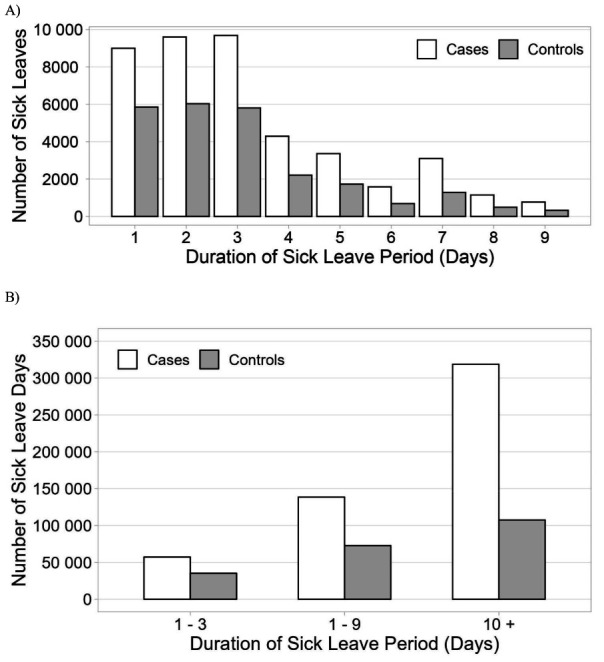
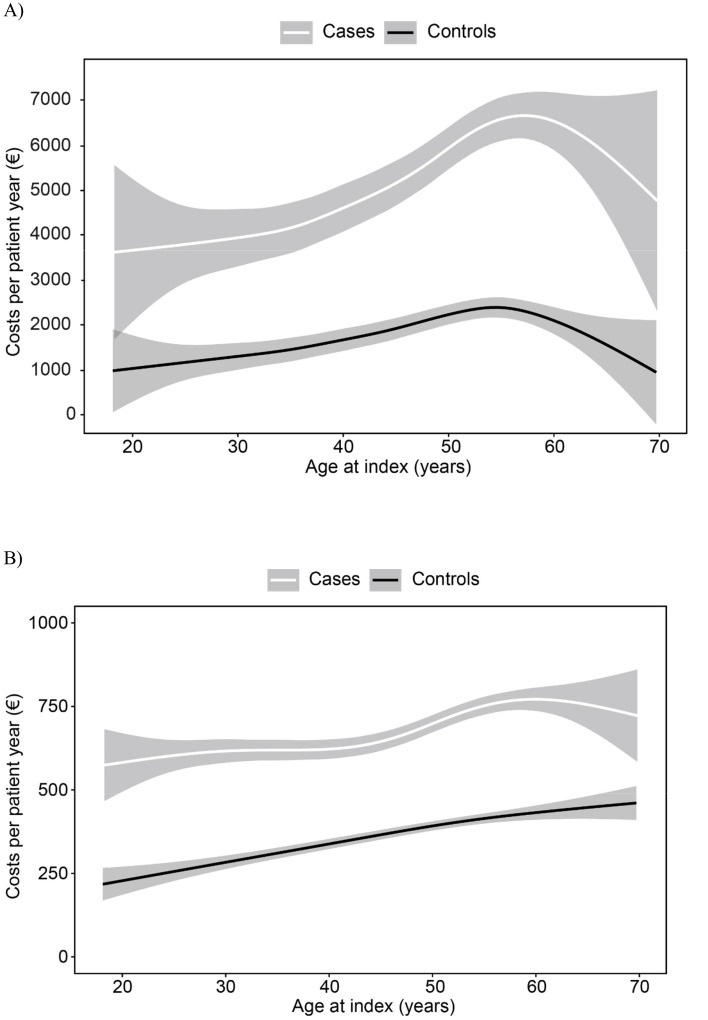
Results: Altogether 5405 patients with IIRD were identified and compared with an equal number of controls. The patients incurred approximately 2.5 times more sick leave than controls: 21.7 versus 8.5 days per patient year, respectively. Short-term sick leave was common: 83% of sickness absence periods of the patients lasted 1-9 days and represented 30% of the total absenteeism. Loss of productivity due to lost workdays was on average €4572 (95% confidence interval €4352-4804) per patient year. Occupational HCRU was approximately 1.8 times higher among IIRD patients than controls.
Conclusions: Workers with an IIRD incur considerably more sick leave and use more occupational healthcare services than controls. Short sick leave not registered in national insurance registers constitute a significant portion of days off work among patients with IIRD.
Conflict of interest statement
AK is employed by Terveystalo, JA, MRa, MRe, and AL are employees of AbbVie and may or may not own AbbVie shares. LUV, MIL, and ST are employed by Medaffcon Oy. MK is a former employee of AbbVie and current employee of Pfizer. KP has no conflicts of interest to declare.
AbbVie sponsored the study; contributed to the design; participated in the collection, analysis, and interpretation of data in writing, reviewing, approving the final version, and decision to submit the paper for publication. No honoraria were made for the authorship.
AK is employed by Terveystalo, JA, MRa, MRe, and AL are employees of AbbVie and may or may not own AbbVie shares. LUV, MIL, and ST are employed by Medaffcon Oy. MK is a former employee of AbbVie and current employee of Pfizer. KP has no conflicts of interest to declare.
Figures
Similar articles
-
Productivity loss outcomes and costs among patients with cholangiocarcinoma in the United States: an economic evaluation.J Med Econ. 2023 Jan-Dec;26(1):454-462. doi: 10.1080/13696998.2023.2187604. J Med Econ. 2023. PMID: 36883994
-
Self-certification versus physician certification of sick leave for reducing sickness absence and associated costs.Cochrane Database Syst Rev. 2019 May 14;5(5):CD013098. doi: 10.1002/14651858.CD013098.pub2. Cochrane Database Syst Rev. 2019. PMID: 31087323 Free PMC article.
-
[Risk factors for absenteeism due to sick leave in the petroleum industry].Rev Saude Publica. 2014 Feb;48(1):103-22. doi: 10.1590/s0034-8910.2014048004609. Rev Saude Publica. 2014. PMID: 24789643 Free PMC article.
-
The economic burden of knee and hip osteoarthritis: absenteeism and costs in the Dutch workforce.BMC Musculoskelet Disord. 2022 Apr 18;23(1):364. doi: 10.1186/s12891-022-05306-9. BMC Musculoskelet Disord. 2022. PMID: 35436874 Free PMC article.
-
[Work absenteeism in Chile according to the type of work place].Rev Med Chil. 2004 Sep;132(9):1100-8. doi: 10.4067/s0034-98872004000900012. Rev Med Chil. 2004. PMID: 15543768 Review. Spanish.
Cited by
-
The association between social determinants of health and all-cause, cardiovascular mortality in US rheumatoid arthritis: a cohort study of NHANES.BMC Public Health. 2025 Apr 22;25(1):1491. doi: 10.1186/s12889-025-22706-3. BMC Public Health. 2025. PMID: 40264100 Free PMC article.
-
Potential of digital applications for self-management and other outcomes in inflammatory rheumatic diseases: a systematic literature review.Front Med (Lausanne). 2025 Jul 9;12:1617151. doi: 10.3389/fmed.2025.1617151. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40703305 Free PMC article.
-
Association between the body roundness index and osteoarthritis: evidence from NHANES.Front Med (Lausanne). 2024 Oct 24;11:1472196. doi: 10.3389/fmed.2024.1472196. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39512614 Free PMC article.
-
Association between dietary retinol intake and rheumatoid arthritis based on NHANES database.BMC Public Health. 2024 Aug 10;24(1):2167. doi: 10.1186/s12889-024-19620-5. BMC Public Health. 2024. PMID: 39127632 Free PMC article.
References
-
- Ajeganova S, van Steenbergen HW, van Nies JA, Burgers LE, Huizinga TW, van der Helm-van Mil AH. Disease-modifying antirheumatic drug-free sustained remission in rheumatoid arthritis: an increasingly achievable outcome with subsidence of disease symptoms. Ann Rheum Dis 2016. May;75(5):867–73. 10.1136/annrheumdis-2014-207080 - DOI - PubMed
-
- Fernández-Carballido C, Tornero C, Castro-Villegas MC, Galindez E, García-Llorente JF, García-Vivar MLet al. ; ESPERANZA study group . No radiographic sacroiliitis progression was observed in patients with early spondyloarthritis at 6 years: results of the Esperanza multicentric prospective cohort. RMD Open 2020. Sep;6(2):e001345. 10.1136/rmdopen-2020-001345 - DOI - PMC - PubMed
-
- Merkesdal S, Ruof J, Schöffski O, Bernitt K, Zeidler H, Mau W. Indirect medical costs in early rheumatoid arthritis: composition of and changes in indirect costs within the first three years of disease. Arthritis Rheum 2001. Mar;44(3):528–34. 10.1002/1529-0131(200103)44:3<528::AID-ANR100>3.0.CO;2-U - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical