

Cerebellar Transcranial Alternating Current Stimulation in Essential Tremor Patients with Thalamic Stimulation: A Proof-of-Concept Study
- PMID: 37097344
- PMCID: PMC10457262
- DOI: 10.1007/s13311-023-01372-6
Cerebellar Transcranial Alternating Current Stimulation in Essential Tremor Patients with Thalamic Stimulation: A Proof-of-Concept Study
Abstract
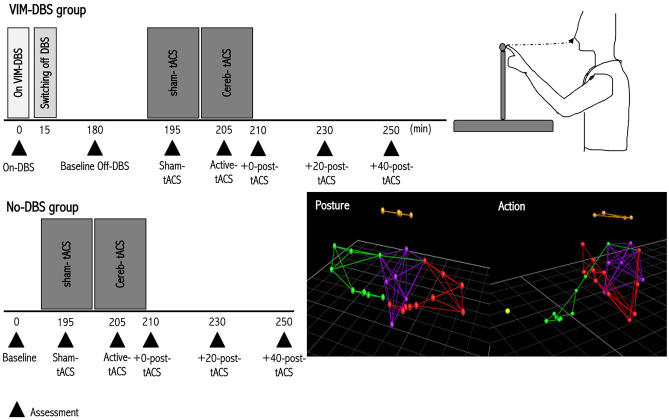
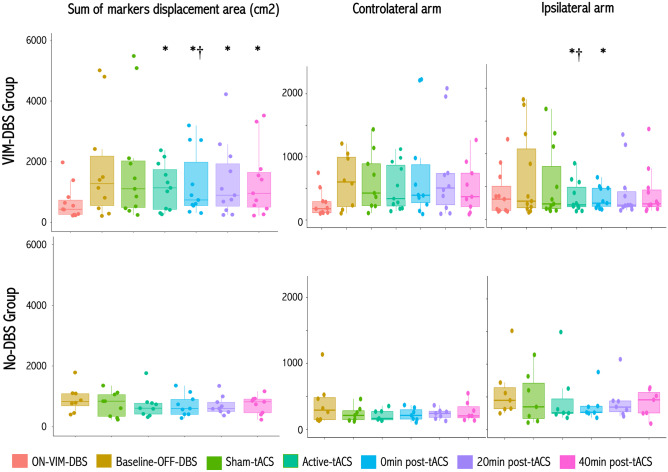
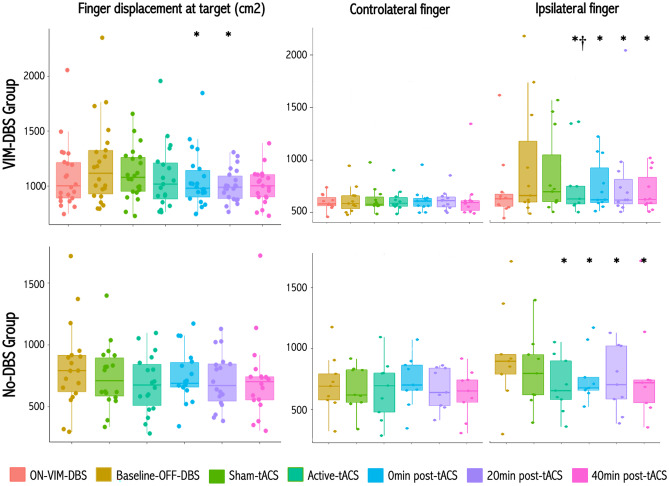
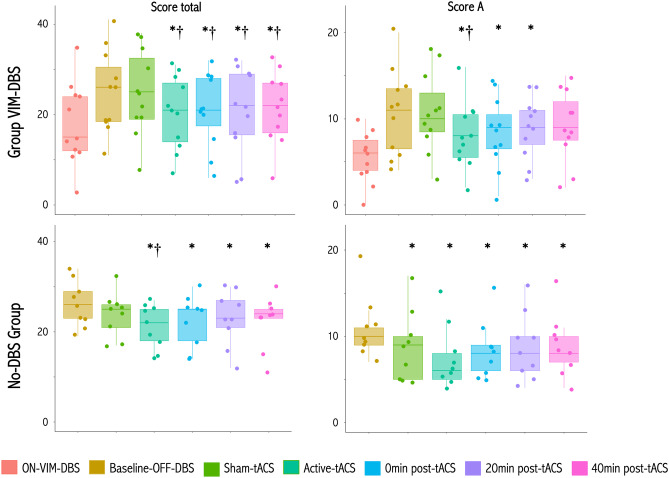
Essential tremor (ET) is a disabling condition resulting from a dysfunction of cerebello-thalamo-cortical circuitry. Deep brain stimulation (DBS) or lesion of the ventral-intermediate thalamic nucleus (VIM) is an effective treatment for severe ET. Transcranial cerebellar brain stimulation has recently emerged as a non-invasive potential therapeutic option. Here, we aim to investigate the effects of high-frequency non-invasive cerebellar transcranial alternating current stimulation (tACS) in severe ET patients already operated for VIM-DBS. Eleven ET patients with VIM-DBS, and 10 ET patients without VIM-DBS and matched for tremor severity, were included in this double-blind proof-of-concept controlled study. All patients received unilateral cerebellar sham-tACS and active-tACS for 10 min. Tremor severity was blindly assessed at baseline, without VIM-DBS, during sham-tACS, during and at 0, 20, 40 min after active-tACS, using kinetic recordings during holding posture and action ('nose-to-target') task and videorecorded Fahn-Tolosa-Marin (FTM) clinical scales. In the VIM-DBS group, active-tACS significantly improved both postural and action tremor amplitude and clinical (FTM scales) severity, relative to baseline, whereas sham-tACS did not, with a predominant effect for the ipsilateral arm. Tremor amplitude and clinical severity were also not significantly different between ON VIM-DBS and active-tACS conditions. In the non-VIM-DBS group, we also observed significant improvements in ipsilateral action tremor amplitude, and clinical severity after cerebellar active-tACS, with a trend for improved postural tremor amplitude. In non-VIM-DBS group, sham- active-tACS also decreased clinical scores. These data support the safety and potential efficacy of high-frequency cerebellar-tACS to reduce ET amplitude and severity.
Keywords: Cerebellum; Deep brain stimulation; Essential tremor; Motion capture; Transcranial alternating current stimulation.
© 2023. The American Society for Experimental Neurotherapeutics, Inc.
Figures
Similar articles
-
Connectivity derived thalamic segmentation in deep brain stimulation for tremor.Neuroimage Clin. 2018 Jan 28;18:130-142. doi: 10.1016/j.nicl.2018.01.008. eCollection 2018. Neuroimage Clin. 2018. PMID: 29387530 Free PMC article.
-
The effect of unilateral thalamic deep brain stimulation on the vocal dysfunction in a patient with spasmodic dysphonia: interrogating cerebellar and pallidal neural circuits.J Neurosurg. 2018 Feb;128(2):575-582. doi: 10.3171/2016.10.JNS161025. Epub 2017 Mar 17. J Neurosurg. 2018. PMID: 28304188 Clinical Trial.
-
Deep brain stimulation of the globus pallidus internus or ventralis intermedius nucleus of thalamus for Holmes tremor.Neurosurg Rev. 2015 Oct;38(4):753-63. doi: 10.1007/s10143-015-0636-0. Epub 2015 May 20. Neurosurg Rev. 2015. PMID: 25990341
-
Reduction in DBS frequency improves balance difficulties after thalamic DBS for essential tremor.J Neurol Sci. 2016 Aug 15;367:122-7. doi: 10.1016/j.jns.2016.06.001. Epub 2016 Jun 2. J Neurol Sci. 2016. PMID: 27423573 Review.
-
Outcomes and Adverse Effects of Deep Brain Stimulation on the Ventral Intermediate Nucleus in Patients with Essential Tremor.Neural Plast. 2020 Aug 1;2020:2486065. doi: 10.1155/2020/2486065. eCollection 2020. Neural Plast. 2020. PMID: 32802034 Free PMC article. Review.
Cited by
-
Essential tremor disrupts rhythmic brain networks during naturalistic movement.Neurobiol Dis. 2025 Apr;207:106858. doi: 10.1016/j.nbd.2025.106858. Epub 2025 Feb 25. Neurobiol Dis. 2025. PMID: 40015653 Free PMC article.
-
Transcranial alternating current stimulation for treating spinocerebellar ataxia type 3: A randomized controlled trial.Cell Rep Med. 2025 Jun 17;6(6):102162. doi: 10.1016/j.xcrm.2025.102162. Cell Rep Med. 2025. PMID: 40532663 Free PMC article. Clinical Trial.
-
Transcranial Alternating Current Stimulation in a Patient with Ataxia-Ocular Apraxia 2: a Case Report.Cerebellum. 2024 Aug;23(4):1713-1717. doi: 10.1007/s12311-023-01637-y. Epub 2023 Nov 22. Cerebellum. 2024. PMID: 37993636
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
