

Lung Recruitment Assessed by Electrical Impedance Tomography (RECRUIT): A Multicenter Study of COVID-19 Acute Respiratory Distress Syndrome
- PMID: 37097986
- PMCID: PMC10870845
- DOI: 10.1164/rccm.202212-2300OC
Lung Recruitment Assessed by Electrical Impedance Tomography (RECRUIT): A Multicenter Study of COVID-19 Acute Respiratory Distress Syndrome
Abstract
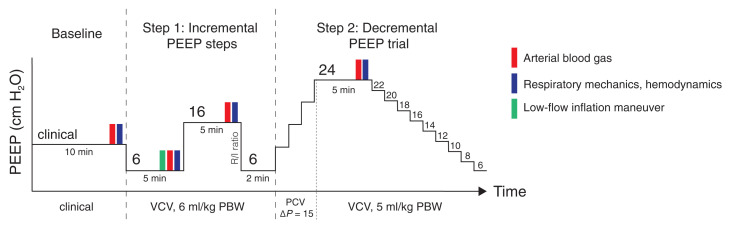
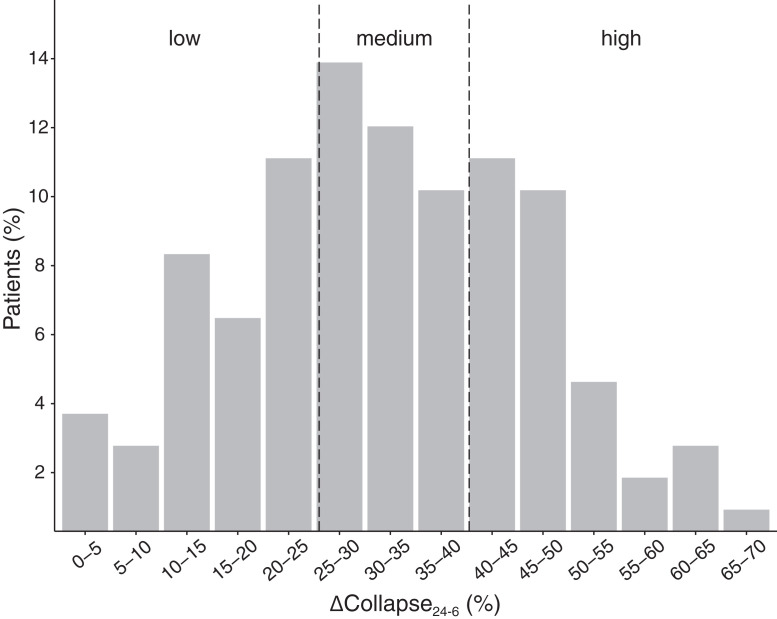
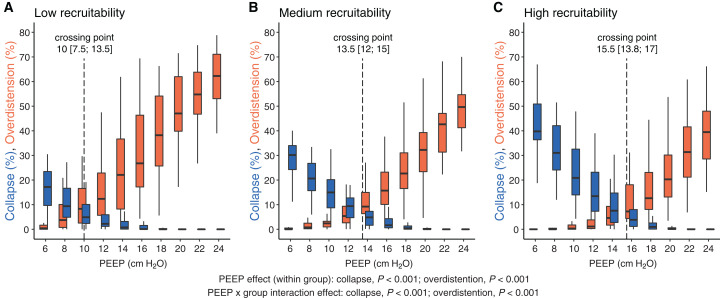
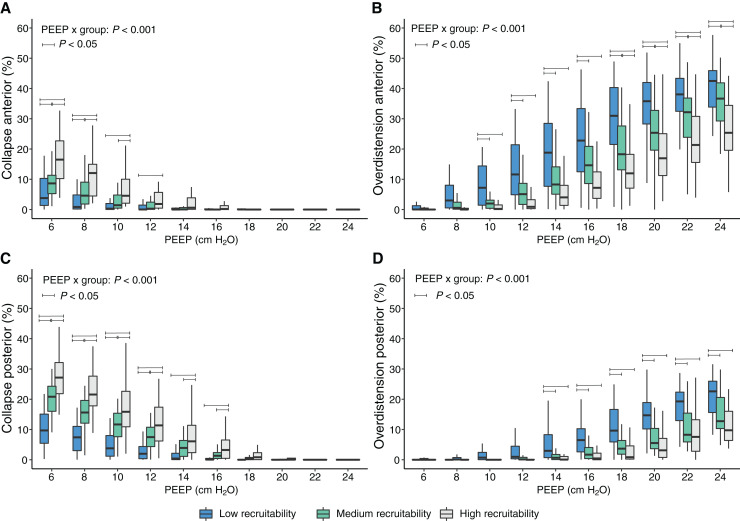
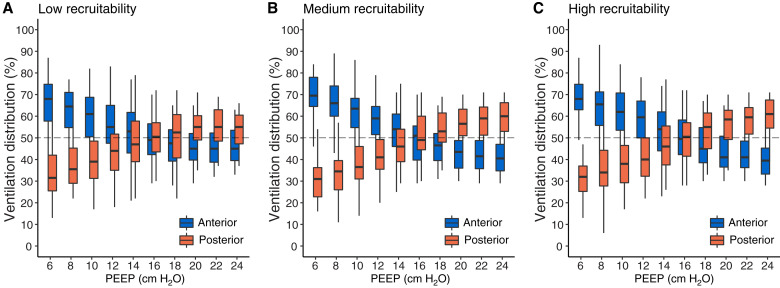
Rationale: Defining lung recruitability is needed for safe positive end-expiratory pressure (PEEP) selection in mechanically ventilated patients. However, there is no simple bedside method including both assessment of recruitability and risks of overdistension as well as personalized PEEP titration. Objectives: To describe the range of recruitability using electrical impedance tomography (EIT), effects of PEEP on recruitability, respiratory mechanics and gas exchange, and a method to select optimal EIT-based PEEP. Methods: This is the analysis of patients with coronavirus disease (COVID-19) from an ongoing multicenter prospective physiological study including patients with moderate-severe acute respiratory distress syndrome of different causes. EIT, ventilator data, hemodynamics, and arterial blood gases were obtained during PEEP titration maneuvers. EIT-based optimal PEEP was defined as the crossing point of the overdistension and collapse curves during a decremental PEEP trial. Recruitability was defined as the amount of modifiable collapse when increasing PEEP from 6 to 24 cm H2O (ΔCollapse24-6). Patients were classified as low, medium, or high recruiters on the basis of tertiles of ΔCollapse24-6. Measurements and Main Results: In 108 patients with COVID-19, recruitability varied from 0.3% to 66.9% and was unrelated to acute respiratory distress syndrome severity. Median EIT-based PEEP differed between groups: 10 versus 13.5 versus 15.5 cm H2O for low versus medium versus high recruitability (P < 0.05). This approach assigned a different PEEP level from the highest compliance approach in 81% of patients. The protocol was well tolerated; in four patients, the PEEP level did not reach 24 cm H2O because of hemodynamic instability. Conclusions: Recruitability varies widely among patients with COVID-19. EIT allows personalizing PEEP setting as a compromise between recruitability and overdistension. Clinical trial registered with www.clinicaltrials.gov (NCT04460859).
Keywords: acute respiratory distress syndrome; electrical impedance tomography; lung recruitability; mechanical ventilation; positive end-expiratory pressure.
Figures


Comment in
-
Electrical Impedance Tomography: The Electrocardiogram for the Lungs?Am J Respir Crit Care Med. 2023 Jul 1;208(1):3-5. doi: 10.1164/rccm.202305-0810ED. Am J Respir Crit Care Med. 2023. PMID: 37311244 Free PMC article. No abstract available.
-
Electrical Impedance Tomography and Optimal Positive End-Expiratory Pressure: Uncovering Latent Heterogeneity of Treatment Effect.Am J Respir Crit Care Med. 2023 Sep 1;208(5):636-637. doi: 10.1164/rccm.202305-0878LE. Am J Respir Crit Care Med. 2023. PMID: 37387585 Free PMC article. No abstract available.
-
Increasing Positive End-Expiratory Pressure to Recruit the Lungs: Take into Account Heart-Lung Interaction and Oxygen Delivery.Am J Respir Crit Care Med. 2023 Sep 1;208(5):637-638. doi: 10.1164/rccm.202305-0891LE. Am J Respir Crit Care Med. 2023. PMID: 37490049 Free PMC article. No abstract available.
References
-
- Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, et al. Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med . 2006;354:1775–1786. - PubMed
-
- Jonkman AH, Ranieri VM, Brochard L. Lung recruitment. Intensive Care Med . 2022;48:936–938. - PubMed
-
- Chiumello D, Marino A, Brioni M, Cigada I, Menga F, Colombo A, et al. Lung recruitment assessed by respiratory mechanics and computed tomography in patients with acute respiratory distress syndrome. What is the relationship? Am J Respir Crit Care Med . 2016;193:1254–1263. - PubMed
-
- Grasso S, Stripoli T, De Michele M, Bruno F, Moschetta M, Angelelli G, et al. ARDSnet ventilatory protocol and alveolar hyperinflation: role of positive end-expiratory pressure. Am J Respir Crit Care Med . 2007;176:761–767. - PubMed
-
- Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med . 2007;175:160–166. - PubMed
