

Association between interpregnancy interval and maternal and neonatal adverse outcomes in women with a cesarean delivery: a population-based study
- PMID: 37098470
- PMCID: PMC10127338
- DOI: 10.1186/s12884-023-05600-x
Association between interpregnancy interval and maternal and neonatal adverse outcomes in women with a cesarean delivery: a population-based study
Abstract
Background: Interpregnancy interval (IPI) has been linked with several maternal and neonatal adverse events in the general population. However, the association between IPI and maternal and neonatal outcomes in women whose first delivery was by cesarean delivery is unclear. We aimed to investigate the association between IPI after cesarean delivery and the risk of maternal and neonatal adverse events.
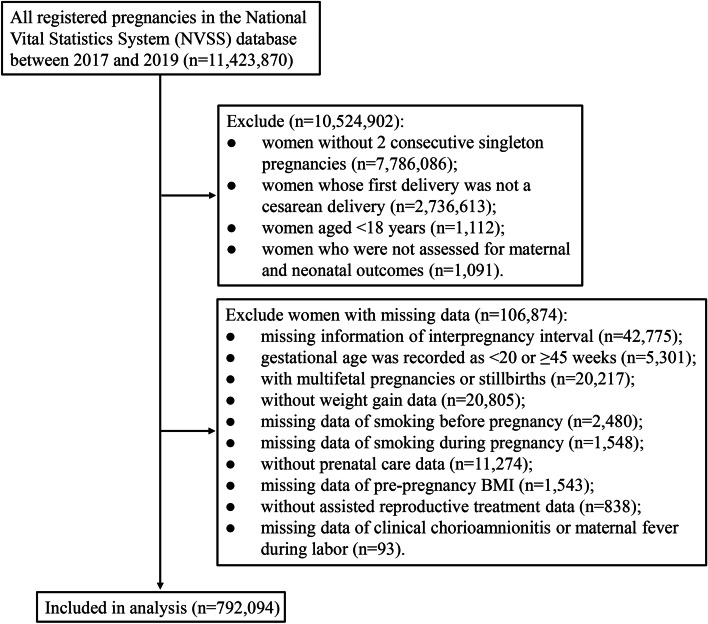
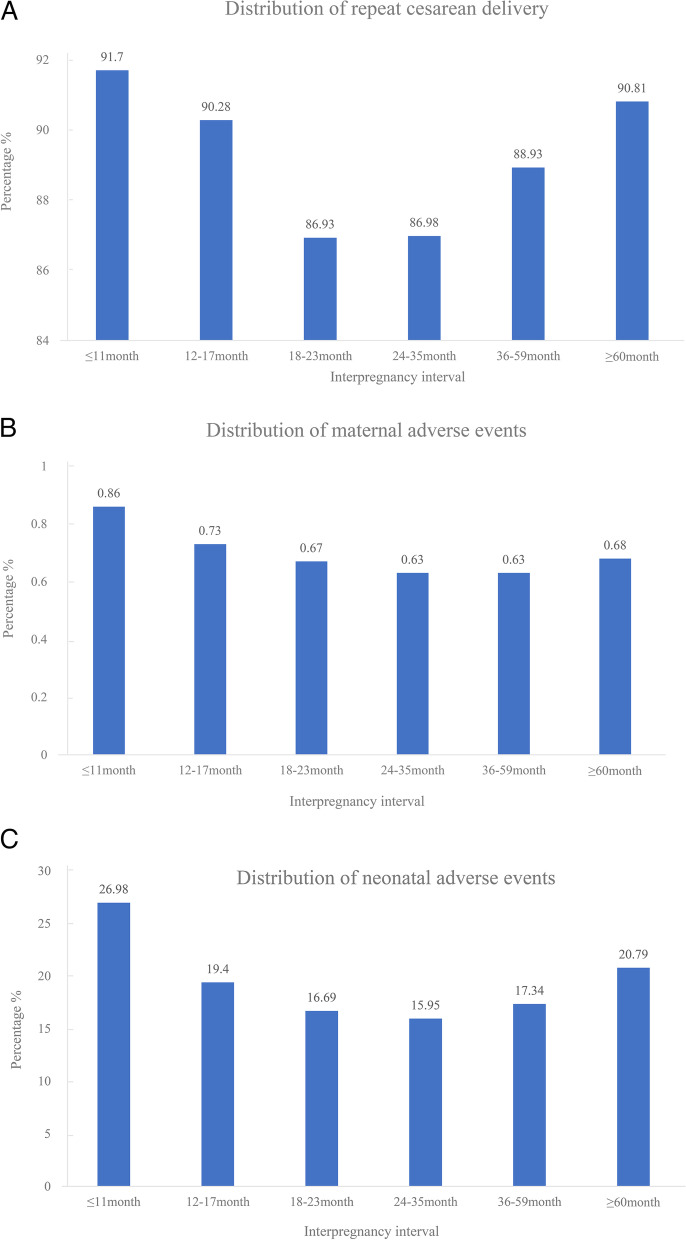
Methods: Women (aged ≥ 18 years) whose first delivery was cesarean delivery with 2 consecutive singleton pregnancies from the National Vital Statistics System (NVSS) database between 2017 and 2019 were included in this retrospective cohort study. In this post-hoc analysis, logistic regression analyses were used to examine IPI (≤ 11, 12-17, 18-23 [reference], 24-35, 36-59, and ≥ 60 months) in relation to the risk of repeat cesarean delivery, maternal adverse events (maternal transfusion, ruptured uterus, unplanned hysterectomy, and admission to an intensive care unit), and neonatal adverse events (low birthweight, premature birth, Apgar score at 5 min < 7, and abnormal conditions of the newborn). Stratified analysis based on age (< 35 and ≥ 35 years) and previous preterm birth.
Results: We included 792,094 maternities, 704,244 (88.91%) of which underwent a repeat cesarean delivery, 5,246 (0.66%) women had adverse events, and 144,423 (18.23%) neonates had adverse events. After adjusting for confounders, compared to an IPI of 18-23 months, the IPI of ≤ 11 months [odds ratio (OR) = 1.55, 95% confidence interval (CI): 1.44-1.66], 12-17 months (OR = 1.38, 95%CI: 1.33-1.43), 36-59 months (OR = 1.12, 95%CI: 1.10-1.15), and ≥ 60 months (OR = 1.19, 95%CI: 1.16-1.22) were associated with an increased risk of repeat cesarean delivery. In terms of maternal adverse events, only IPI of ≥ 60 months (OR = 0.85, 95%CI: 0.76-0.95) was observed to be associated with decreased risk of maternal adverse events in women aged < 35 years. In analysis of neonatal adverse events, IPI of ≤ 11 months (OR = 1.14, 95%CI: 1.07-1.21), 12-17 months (OR = 1.07, 95%CI: 1.03-1.10), and ≥ 60 months (OR = 1.05, 95%CI: 1.02-1.08) were related to an increased risk of neonatal adverse events.
Conclusion: Both short and long IPI were associated with an increased risk of repeat cesarean delivery and neonatal adverse events, and women < 35 years may benefit from a longer IPI.
Keywords: Cesarean delivery; Interpregnancy interval; Maternal outcome; Neonatal events.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Association between interpregnancy interval and adverse perinatal outcomes among subsequent twin pregnancies: a nationwide population-based study.Am J Obstet Gynecol MFM. 2024 Sep;6(9):101439. doi: 10.1016/j.ajogmf.2024.101439. Epub 2024 Jul 28. Am J Obstet Gynecol MFM. 2024. PMID: 39079615
-
Twin pregnancy following a short interpregnancy interval: Maternal and neonatal outcomes.Eur J Obstet Gynecol Reprod Biol. 2022 Sep;276:185-190. doi: 10.1016/j.ejogrb.2022.07.026. Epub 2022 Jul 29. Eur J Obstet Gynecol Reprod Biol. 2022. PMID: 35930813
-
Association between interpregnancy interval and adverse perinatal outcomes according to maternal age in the context of China's two-child policy.BMC Pregnancy Childbirth. 2025 Jan 27;25(1):81. doi: 10.1186/s12884-025-07136-8. BMC Pregnancy Childbirth. 2025. PMID: 39871180 Free PMC article.
-
Short interpregnancy interval and adverse birth outcomes in women of advanced age: a population-based study.Ann Epidemiol. 2018 Sep;28(9):605-611. doi: 10.1016/j.annepidem.2018.06.007. Epub 2018 Jun 22. Ann Epidemiol. 2018. PMID: 30006251
-
Interpregnancy interval and obstetrical complications.Obstet Gynecol Surv. 2012 Sep;67(9):584-96. doi: 10.1097/OGX.0b013e31826b2c3e. Obstet Gynecol Surv. 2012. PMID: 22990461 Review.
Cited by
-
Inter-pregnancy interval and uterine rupture during a trial of labour after one previous caesarean delivery and no previous vaginal births: a retrospective population-based cohort study.EClinicalMedicine. 2025 Jan 21;80:103071. doi: 10.1016/j.eclinm.2025.103071. eCollection 2025 Feb. EClinicalMedicine. 2025. PMID: 39902314 Free PMC article.
-
Non-linear association between interpregnancy interval after vaginal delivery and singleton preterm birth: a retrospective cohort study.BMC Pregnancy Childbirth. 2025 Mar 11;25(1):275. doi: 10.1186/s12884-025-07373-x. BMC Pregnancy Childbirth. 2025. PMID: 40069651 Free PMC article.
References
-
- Kangatharan C, Labram S, Bhattacharya S. Interpregnancy interval following miscarriage and adverse pregnancy outcomes: systematic review and meta-analysis. Hum Reprod Update. 2017;23:221–231. - PubMed
-
- DeFranco EA, Seske LM, Greenberg JM, Muglia LJ. Influence of interpregnancy interval on neonatal morbidity. Am J Obstet Gynecol. 2015;212(386):e1–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
