

Disparities and barriers of health facility delivery following optimal and suboptimal pregnancy care in Nigeria: evidence of home births from cross-sectional surveys
- PMID: 37098533
- PMCID: PMC10131351
- DOI: 10.1186/s12905-023-02364-6
Disparities and barriers of health facility delivery following optimal and suboptimal pregnancy care in Nigeria: evidence of home births from cross-sectional surveys
Abstract
Background: Despite uptake of antenatal care (ANC), 70% of global burden of maternal and child mortality is prevalent in sub-Saharan Africa, particularly Nigeria, due to persistent home delivery. Thus, this study investigated the disparity and barriers to health facility delivery and the predictors of home delivery following optimal and suboptimal uptake of ANC in Nigeria.
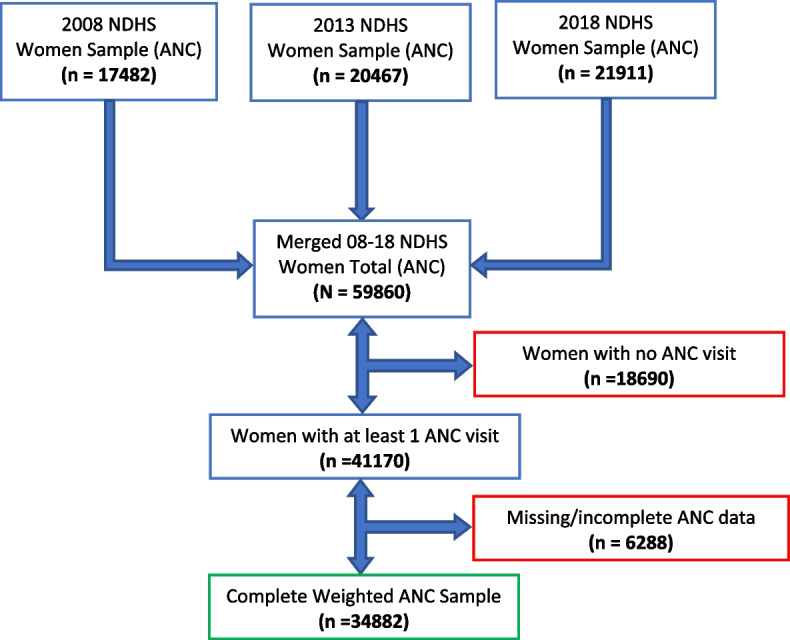
Methodology: A secondary analysis of 34882 data from 3 waves of cross-sectional surveys (2008-2018 NDHS). Home delivery is the outcome while explanatory variables were classified as socio-demographics, obstetrics, and autonomous factors. Descriptive statistics (bar chart) reported frequencies and percentages of categorical data, median (interquartile range) summarized the non-normal count data. Bivariate chi-square test assessed relationship at 10% cutoff point (p < 0.10) and median test examined differences in medians of the non-normal data in two groups. Multivariable logistic regression (Coeff plot) evaluated the likelihood and significance of the predictors at p < 0.05.
Results: 46.2% of women had home delivery after ANC. Only 5.8% of women with suboptimal ANC compared to the 48.0% with optimal ANC had facility delivery and the disparity was significant (p < 0.001). Older maternal age, SBA use, joint health decision making and ANC in a health facility are associated with facility delivery. About 75% of health facility barriers are due to high cost, long distance, poor service, and misconceptions. Women with any form of obstacle utilizing health facility are less likely to receive ANC in a health facility. Problem getting permission to seek for medical help (aOR = 1.84, 95%CI = 1.20-2.59) and religion (aOR = 1.43, 95%CI = 1.05-1.93) positively influence home delivery after suboptimal ANC while undesired pregnancy (aOR = 1.27, 95%CI = 1.01-1.60) positively influence home delivery after optimal ANC. Delayed initiation of ANC (aOR = 1.19, 95%CI = 1.02-1.39) is associated with home delivery after any ANC.
Conclusions: About half of women had home delivery after ANC. Hence disparity exist between suboptimal and optimal ANC attendees in institutional delivery. Religion, unwanted pregnancy, and women autonomy problem raise the likelihood of home delivery. Four-fifth of health facility barriers can be eradicated by optimizing maternity package with health education and improved quality service that expand focus ANC to capture women with limited access to health facility.
Keywords: Antenatal care; Healthcare facility; Home delivery; Multivariable regression; Women.
© 2023. The Author(s).
Conflict of interest statement
The author declare no competing interests.
Figures


References
-
- Ama NO, Ngome E. Challenges faced by older women in Botswana in accessing services that address sexual and reproductive health, and family planning needs. Botswana South African Fam Pract. 2013;55(3):281–288. doi: 10.1080/20786204.2013.10874351. - DOI
-
- Robert E. Black, Neff Walker, Ramanan Laxminarayan and MT. Reproductive, Maternal, Newborn, and Child Health 2 VOLUME DISEASE CONTROL PRIORITIES • THIRD EDITION. 2020;2:419. - PubMed
-
- Kifle D, Azale T, Gelaw YA, Melsew YA. Maternal health care service seeking behaviors and associated factors among women in rural Haramaya District, Eastern Ethiopia: a triangulated community-based cross-sectional study. Reprod Health. 2017;14(1):1–11. doi: 10.1186/s12978-016-0270-5. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
