

Breast implant associated EBV-positive Diffuse Large B-cell lymphoma: an underrecognized entity?
- PMID: 37098615
- PMCID: PMC10127423
- DOI: 10.1186/s13000-023-01337-5
Breast implant associated EBV-positive Diffuse Large B-cell lymphoma: an underrecognized entity?
Abstract
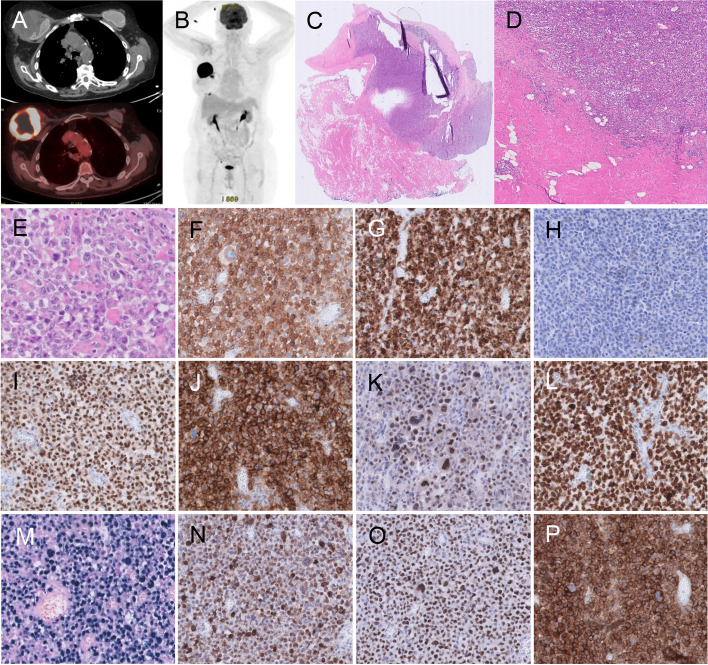
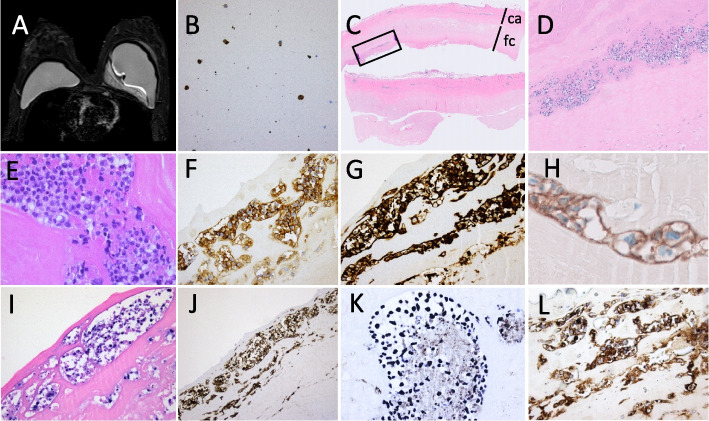
Breast-implant associated (BIA) lymphoma is an infrequent type of cancer occurring in the fluid and fibrous capsule around a textured breast implant. Recently, both the 2022 WHO 5th edition classification of Haematological tumours (WHO HAEM5) and 2022 International Consensus Classification of Mature Lymphoid Neoplasms (22ICC), recognized breast implant-associated Anaplastic Large Cell Lymphoma (BIA-ALCL) as a definitive entity, defined as a mature CD30-positive T-cell lymphoma, confined by a fibrous capsule, in a breast implant setting. Only few B-cell lymphomas have been reported in the literature to be associated with breast implants. Here we report two EBV-positive Diffuse Large B-cell lymphomas (EBV + DLBCL) in relation to a breast implant, both expressing CD30 as well as EBV latency type 3. Both lesions were considered as DLBCL associated with chronic inflammation (CI-DLBCL), but one presented as a 7 cm solid mass, while the other presented as a fibrin-associated DLBCL (FA-DLBCL) in an HIV patient. Clinically, both are in complete remission 6 months or longer after capsulectomy and graft removal, without additional chemotherapy.Such cases, characterized by large CD30-positive cells, can easily be misdiagnosed as BIA-ALCL if the cell of origin is not further established. Therefore, a diagnostic panel including lineage-specific B-and T-cell markers and EBER in situ hybridization is essential to recognize this rare entity, to understand lymphomagenesis, to predict outcome and to define clinical approach.
Keywords: BIA-DLBCL; Breast implant associated lymphoma; CI-DLBCL; EBV + DLBCL; FA-DLBCL.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
