

Improvement of vertebral body fracture reduction utilizing a posterior reduction tool: a single-center experience
- PMID: 37098619
- PMCID: PMC10131469
- DOI: 10.1186/s13018-023-03793-7
Improvement of vertebral body fracture reduction utilizing a posterior reduction tool: a single-center experience
Abstract
Background: Extensive research regarding instabilities and prevention of kyphotic malalignment in the thoracolumbar spine exists. Keystones of this treatment are posterior instrumentation and anterior vertebral height restoration. Anterior column reduction via a single-stage procedure seems to be advantageous regarding complication, blood loss, and OR-time. Mechanical elevation of the anterior cortex of the vertebra may prevent the necessity of additional anterior stabilization or vertebral body replacement. The purpose of this study was to examine (1) if increased bony reduction in the anterior vertebral cortex could be achieved by utilization of an additional reduction tool, (2) if postoperative loss of vertebral height could be reduced, and (3) if anterior column reduction is related to clinical outcome.
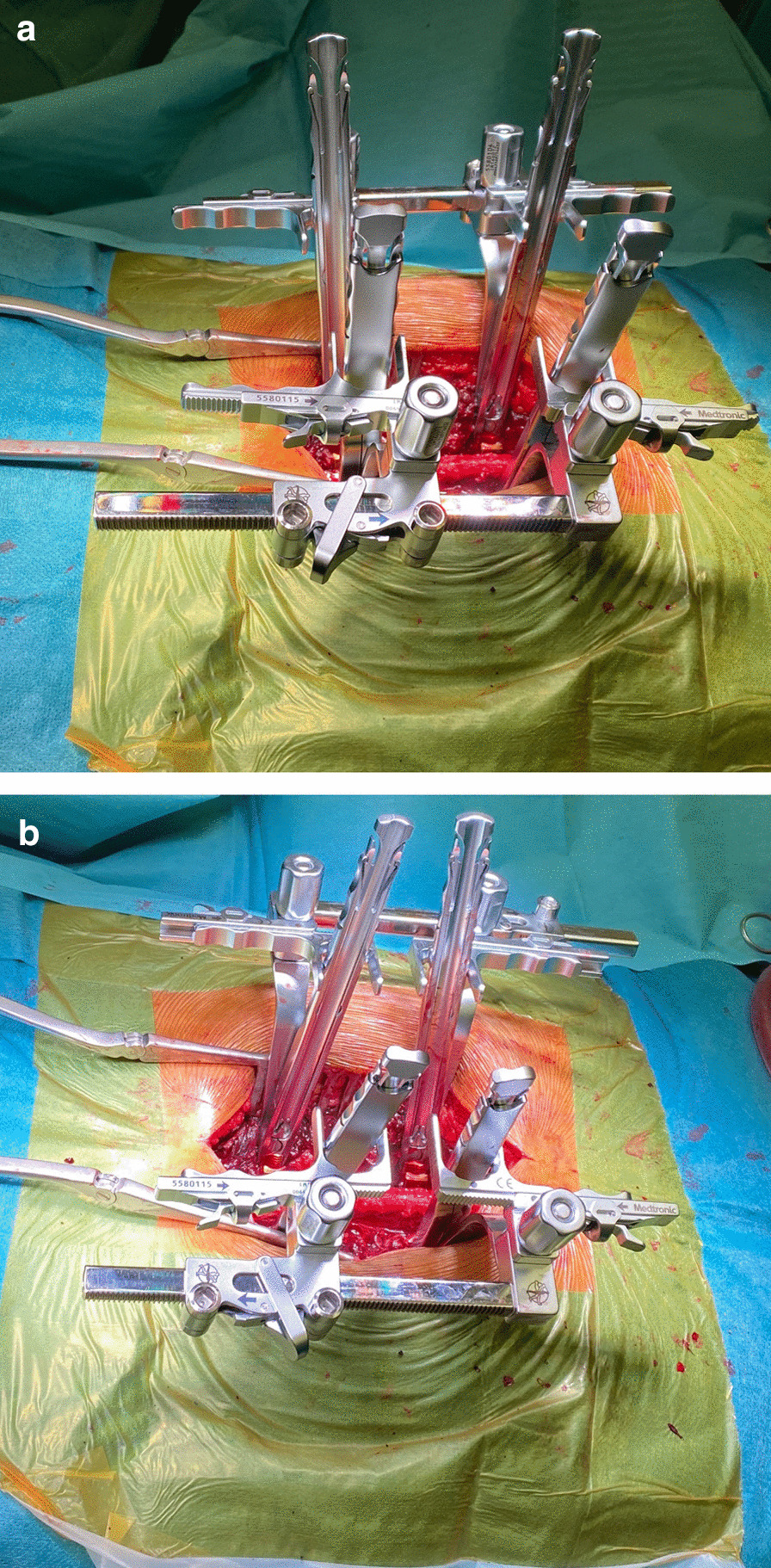
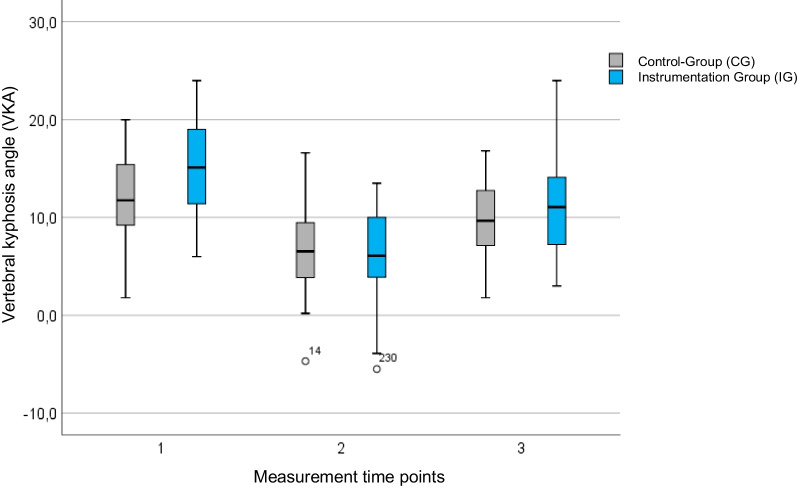
Methods: From one level I trauma center, 173 patients underwent posterior stabilization for fractures of the thoracolumbar region between 2015 and 2020. Reduction in the vertebral body was performed via intraoperative lordotic positioning or by utilization of an additional reduction tool (Nforce, Medtronic). The reduction tool was mounted onto the pedicle screws and removed after tightening of the locking screws. To assess bony reduction, the sagittal index (SI) and vertebral kyphosis angle (VKA) were measured on X-rays and CT images at different time points ((1) preoperative, (2) postoperative, (3) ≥ 3 months postoperative). Clinical outcome was assessed utilizing the Ostwestry Disability Index (ODI).
Results: Bisegmental stabilization of AO/OTA type A3/A4 vertebral fractures was performed in 77 patients. Thereof, reduction was performed in 44 patients (females 34%) via intraoperative positioning alone (control group), whereas 33 patients (females 33%) underwent additional reduction utilizing a mechanical reduction tool (instrumentation group). Mean age was 41 ± 13 years in the instrumentation group (IG) and 52 ± 12 years in the control group (CG) (p < 0.001). No differences in terms of gender and comorbidities were found between the two groups. Preoperatively, the sagittal index (SI) was 0.69 in IG compared to 0.74 in CG (p = 0.039), resulting in a vertebral kyphosis angle (VKA) of 15.0° vs. 11.7° (p = 0.004). Intraoperatively, a significantly greater correction of the kyphotic deformity was achieved in the IG (p < 0.001), resulting in a compensation of the initially more severe kyphotic malalignment. The SI was corrected by 0.20-0.88 postoperatively, resulting in an improvement of the VKA by 8.7°-6.3°. In the CG, the SI could be corrected by 0.12-0.86 and the VKA by 5.1°-6.6°. The amount of correction was influenced by the initial deformity (p < 0.001). Postoperatively, both groups showed a loss of correction, resulting in a gain of 0.08 for the SI and 4.1° in IG and 0.03 and 2.0°, respectively. The best results were observed in younger patients with initially severe kyphotic deformity. Considering various influencing factors, clinical outcome determined by the ODI showed no significant differences between both groups.
Conclusion: Utilization of the investigated reduction tool during posterior stabilization of vertebral body fractures in a suitable collective of young patients with good bone quality and severe fracture deformity may lead to better reduction in the ventral column of the fractured vertebral body and angle correction. Therefore, additional anterior stabilization or vertebral body replacement may be prevented.
Keywords: Posterior surgical treatment; Reduction tool; Thoracolumbar spine; Vertebral fracture.
© 2023. The Author(s).
Conflict of interest statement
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Figures




Similar articles
-
Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedicle-screw instrumentation and fusion.Spine (Phila Pa 1976). 2008 Feb 15;33(4):E100-8. doi: 10.1097/BRS.0b013e3181646b07. Spine (Phila Pa 1976). 2008. PMID: 18277858
-
Monosegmental anterior column reconstruction using an expandable vertebral body replacement device in combined posterior-anterior stabilization of thoracolumbar burst fractures.Arch Orthop Trauma Surg. 2018 Jul;138(7):939-951. doi: 10.1007/s00402-018-2926-9. Epub 2018 Apr 6. Arch Orthop Trauma Surg. 2018. PMID: 29623406 Free PMC article.
-
Is restoration of vertebral body height after vertebral body fractures and minimally-invasive dorsal stabilization with polyaxial pedicle screws just an illusion?Arch Orthop Trauma Surg. 2024 Jan;144(1):239-250. doi: 10.1007/s00402-023-05082-8. Epub 2023 Oct 15. Arch Orthop Trauma Surg. 2024. PMID: 37838983 Free PMC article.
-
Isolated unstable burst fractures of the fifth lumbar vertebra: functional and radiological outcome after posterior stabilization with reconstruction of the anterior column: About 6 cases and literature review.Orthop Traumatol Surg Res. 2020 Oct;106(6):1215-1220. doi: 10.1016/j.otsr.2020.03.014. Epub 2020 Apr 27. Orthop Traumatol Surg Res. 2020. PMID: 32354682 Review.
-
Single-stage posterior vertebral column resection and internal fixation for old fracture-dislocations of thoracolumbar spine: a case series and systematic review.Eur Spine J. 2016 Aug;25(8):2497-513. doi: 10.1007/s00586-015-3955-5. Epub 2015 May 8. Eur Spine J. 2016. PMID: 25953526
Cited by
-
The validity of posterior approach in thoracolumbar spine fracture surgery: A study of 104 cases with literature review.J Craniovertebr Junction Spine. 2025 Apr-Jun;16(2):212-217. doi: 10.4103/jcvjs.jcvjs_50_25. Epub 2025 Jul 3. J Craniovertebr Junction Spine. 2025. PMID: 40756500 Free PMC article.
References
-
- Reinhold M, Knop C, Beisse R, et al. [Operative treatment of traumatic fractures of the thoracic and lumbar spinal column: Part III: Follow up data] [Operative treatment of traumatic fractures of the thorax and lumbar spine. Part II: surgical treatment and radiological findings]. [Operative treatment of traumatic fractures of the thoracic and lumbar spinal column. Part I: epidemiology]. Unfallchirurg. 2009;112(3):294–316. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
