

Peri-Intubation Adverse Events in the Critically Ill Child After Hematopoietic Cell Transplant
- PMID: 37098779
- PMCID: PMC10330041
- DOI: 10.1097/PCC.0000000000003243
Peri-Intubation Adverse Events in the Critically Ill Child After Hematopoietic Cell Transplant
Abstract
Objectives: Mechanically ventilated children post-hematopoietic cell transplant (HCT) have increased morbidity and mortality compared with other mechanically ventilated critically ill children. Tracheal intubation-associated adverse events (TIAEs) and peri-intubation hypoxemia universally portend worse outcomes. We investigated whether adverse peri-intubation associated events occur at increased frequency in patients with HCT compared with non-HCT oncologic or other PICU patients and therefore might contribute to increased mortality.
Design: Retrospective cohort between 2014 and 2019.
Setting: Single-center academic noncardiac PICU.
Patients: Critically ill children who underwent tracheal intubation (TI).
Interventions: None.
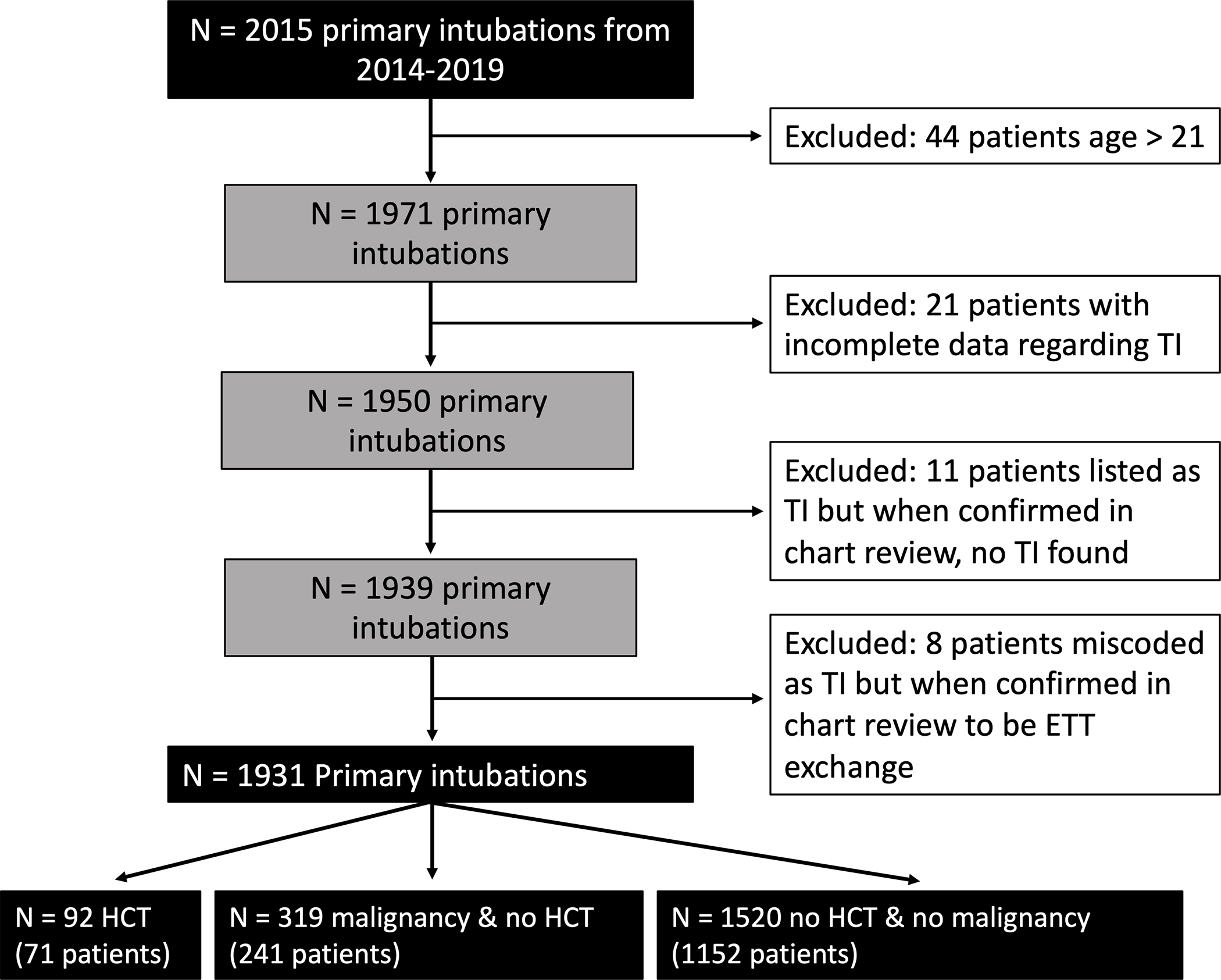
Measurements and main results: Data from the local airway management quality improvement databases and Virtual Pediatric Systems were merged. These data were supplemented with a retrospective chart review for HCT-related data, including HCT indication, transplant-related comorbidity status, and patient condition at the time of TI procedure. The primary outcome was defined as the composite of hemodynamic TIAE (hypo/hypertension, arrhythmia, cardiac arrest) and/or peri-intubation hypoxemia (oxygen saturation < 80%) events. One thousand nine hundred thirty-one encounters underwent TI, of which 92 (4.8%) were post-HCT, while 319 (16.5%) had history of malignancy without HCT, and 1,520 (78.7%) had neither HCT nor malignancy. Children post-HCT were older more often had respiratory failure as an indication for intubation, use of catecholamine infusions peri-intubation, and use of noninvasive ventilation prior to intubation. Hemodynamic TIAE or peri-intubation hypoxemia were not different across three groups (HCT 16%, non-HCT with malignancy 10%, other 15). After adjusting for age, difficult airway feature, provider type, device, apneic oxygenation use, and indication for intubation, we did not identify an association between HCT status and the adverse TI outcome (odds ratio, 1.32 for HCT status vs other; 95% CI, 0.72-2.41; p = 0.37).
Conclusions: In this single-center study, we did not identify an association between HCT status and hemodynamic TIAE or peri-intubation hypoxemia during TI.
Copyright © 2023 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Nishisaki’s and Mrs. Napolitano’s institutions received funding from the Agency for Healthcare Research and Quality (AHRQ) (R18HS024511). Dr. Nishisaki’s institution received funding from Critical Care Medicine and Chiesi; she received support for article research from the AHRQ. Dr. Lindell is supported by the Thrasher Research Fund. Dr. Fitzgerald is supported by National Institutes of Health (NIH) National Institute of Digestive and Diabetes and Kidney Diseases (K23DK119463). Drs. Yehya’s and Fitzgerald’s institutions received funding from NIH. Dr. Yehya’s institution received funding from Pfizer. Drs. Yehya and Rowan received support for article research from the NIH. Ms. Napolitano’s institution received funding from Dräger, Timpel, Philips/Respironics, Actuated Medical, and VERO-Biotech. Dr. Rowan’s institution received funding from the National Heart, Lung, and Blood Institute (K23HL150244). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Chima RJ, Daniels RC, Kim MO, et al. Improved outcomes for stem cell transplant recipients requiring pediatric intensive care. Pediatr Crit Car Med 2012;13(6): 336–e34 - PubMed
-
- Lindell RB, Gertz SJ, Rowan CM, et al. High Levels of Morbidity and Mortality Among Pediatric Hematopoietic Cell Transplant Recipients With Severe Sepsis: Insights From the Sepsis PRevalence, OUtcomes, and Therapies International Point Prevalence Study. Pediatr Crit Care Med 2017;18(12):1114–112 - PMC - PubMed
-
- Jacobe SJ, Hassan A, Veys P, Mok Q. Outcome of children requiring admission to an intensive care unit after bone marrow transplantation. Crit Care Med 2003;31(5):1299–1305. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
