

Efficacy and Safety of Intraoperative Hyperthermic Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer: A Phase 3 Randomized Clinical Trial
- PMID: 37099280
- PMCID: PMC10134040
- DOI: 10.1001/jamasurg.2023.0662
Efficacy and Safety of Intraoperative Hyperthermic Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer: A Phase 3 Randomized Clinical Trial
Abstract
Importance: Peritoneal metastasis in patients with locally advanced colon cancer (T4 stage) is estimated to recur at a rate of approximately 25% at 3 years from surgical resection and is associated with poor prognosis. There is controversy regarding the clinical benefit of prophylactic hyperthermic intraperitoneal chemotherapy (HIPEC) in these patients.
Objective: To assess the efficacy and safety of intraoperative HIPEC in patients with locally advanced colon cancer.
Design, setting, and participants: This open-label, phase 3 randomized clinical trial was conducted in 17 Spanish centers from November 15, 2015, to March 9, 2021. Enrolled patients were aged 18 to 75 years with locally advanced primary colon cancer diagnosed preoperatively (cT4N02M0).
Interventions: Patients were randomly assigned 1:1 to receive cytoreduction plus HIPEC with mitomycin C (30 mg/m2 over 60 minutes; investigational group) or cytoreduction alone (comparator group), both followed by systemic adjuvant chemotherapy. Randomization of the intention-to-treat population was done via a web-based system, with stratification by treatment center and sex.
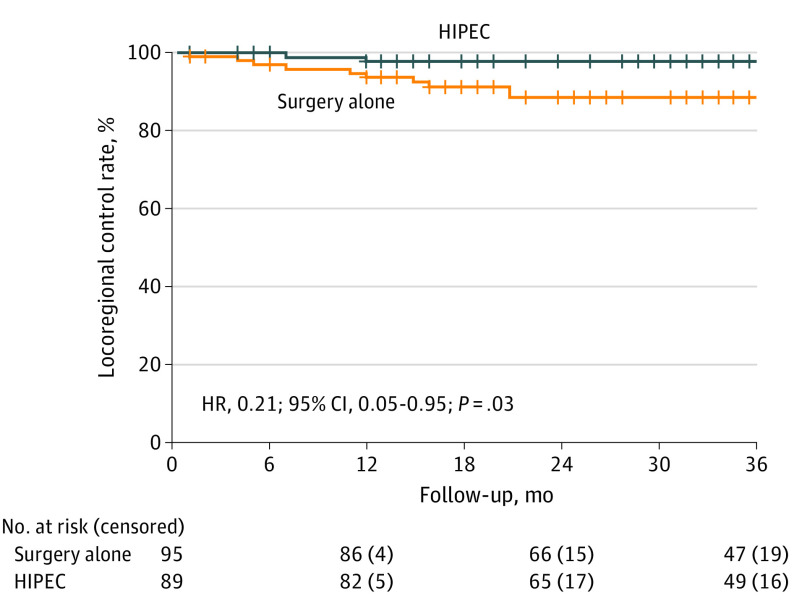
Main outcomes and measures: The primary outcome was 3-year locoregional control (LC) rate, defined as the proportion of patients without peritoneal disease recurrence analyzed by intention to treat. Secondary end points were disease-free survival, overall survival, morbidity, and rate of toxic effects.
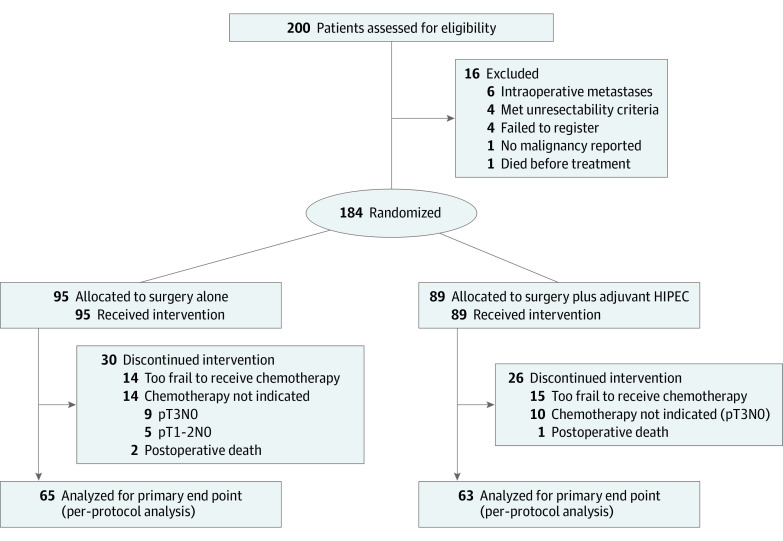
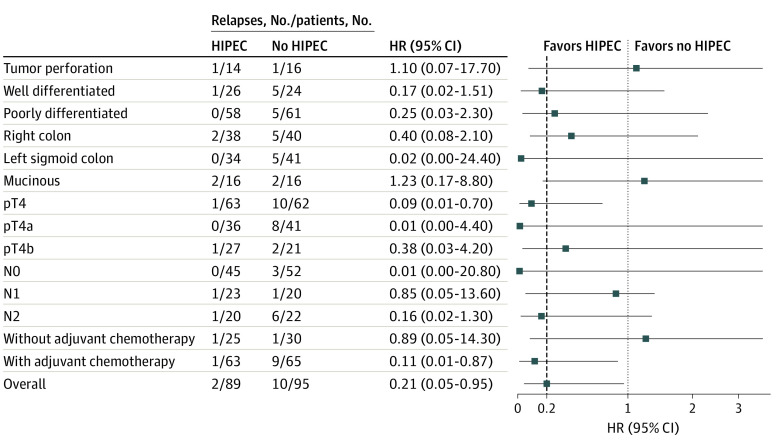
Results: A total of 184 patients were recruited and randomized (investigational group, n = 89; comparator group, n = 95). The mean (SD) age was 61.5 (9.2) years, and 111 (60.3%) were male. Median duration of follow-up was 36 months (IQR, 27-36 months). Demographic and clinical characteristics were similar between groups. The 3-year LC rate was higher in the investigational group (97.6%) than in the comparator group (87.6%) (log-rank P = .03; hazard ratio [HR], 0.21; 95% CI, 0.05-0.95). No differences were observed in disease-free survival (investigational, 81.2%; comparator, 78.0%; log-rank P = .22; HR, 0.71; 95% CI, 0.41-1.22) or overall survival (investigational, 91.7%; comparator, 92.9%; log-rank P = .68; HR, 0.79; 95% CI, 0.26-2.37). The definitive subgroup with pT4 disease showed a pronounced benefit in 3-year LC rate after investigational treatment (investigational: 98.3%; comparator: 82.1%; log-rank P = .003; HR, 0.09; 95% CI, 0.01-0.70). No differences in morbidity or toxic effects between groups were observed.
Conclusions and relevance: In this randomized clinical trial, the addition of HIPEC to complete surgical resection for locally advanced colon cancer improved the 3-year LC rate compared with surgery alone. This approach should be considered for patients with locally advanced colorectal cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT02614534.
Conflict of interest statement
Figures
Comment in
-
Heated Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer-Restarting the Fire.JAMA Surg. 2023 Jul 1;158(7):692. doi: 10.1001/jamasurg.2023.0677. JAMA Surg. 2023. PMID: 37099277 No abstract available.
-
Efficacy, Safety, and Analysis Issues in a Study of Intraoperative Hyperthermic Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer.JAMA Surg. 2023 Dec 1;158(12):1356-1357. doi: 10.1001/jamasurg.2023.3480. JAMA Surg. 2023. PMID: 37585195 No abstract available.
-
Efficacy, Safety, and Analysis Issues in a Study of Intraoperative Hyperthermic Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer.JAMA Surg. 2023 Dec 1;158(12):1357-1358. doi: 10.1001/jamasurg.2023.3483. JAMA Surg. 2023. PMID: 37585200 No abstract available.
References
-
- Franko J, Shi Q, Meyers JP, et al. ; Analysis and Research in Cancers of the Digestive System (ARCAD) Group . Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. Lancet Oncol. 2016;17(12):1709-1719. doi: 10.1016/S1470-2045(16)30500-9 - DOI - PubMed
-
- Verwaal VJ, van Ruth S, de Bree E, et al. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol. 2003;21(20):3737-3743. doi: 10.1200/JCO.2003.04.187 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
