

What Changes Have Occurred in Opioid Prescriptions and the Prescribers of Opioids Before TKA and THA? A Large National Registry Study
- PMID: 37099415
- PMCID: PMC10427048
- DOI: 10.1097/CORR.0000000000002653
What Changes Have Occurred in Opioid Prescriptions and the Prescribers of Opioids Before TKA and THA? A Large National Registry Study
Abstract
Background: Opioid use before TKA or THA is linked to a higher risk of revision surgery and less functional improvement. In Western countries, the frequency of preoperative opioid use has varied, and robust information on temporal changes in opioid prescriptions over time (in the months before surgery as well as annual changes) and among prescribers is necessary to pinpoint opportunities to improve on low-value care patterns, and when they are recognized, to target physician populations for intervention strategies.
Questions/purposes: (1) What proportion of patients undergoing arthroplasties receive an opioid prescription in the year before TKA or THA, and what were the preoperative opioid prescription rates over time between 2013 and 2018? (2) Does the preoperative prescription rate vary between 12 and 10 months and between 3 and 1 months in the year before TKA or THA, and did it change between 2013 and 2018? (3) Which medical professionals were the main prescribers of preoperative opioids 1 year before TKA or THA?
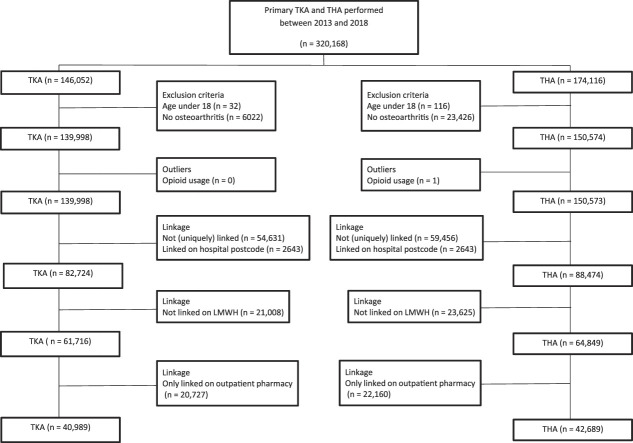
Methods: This was a large-database study drawn from longitudinally maintained national registry sources in the Netherlands. The Dutch Foundation for Pharmaceutical Statistics was linked to the Dutch Arthroplasty Register from 2013 to 2018. TKAs and THAs performed because of osteoarthritis in patients older than 18 years, which were also uniquely linked by age, gender, patient postcode, and low-molecular weight heparin use, were eligible. Between 2013 and 2018, 146,052 TKAs were performed: 96% (139,998) of the TKAs were performed for osteoarthritis in patients older than 18 years; of them, 56% (78,282) were excluded because of our linkage criteria. Some of the linked arthroplasties could not be linked to a community pharmacy, which was necessary to follow patients over time, leaving 28% (40,989) of the initial TKAs as our study population. Between 2013 and 2018, 174,116 THAs were performed: 86% (150,574) were performed for osteoarthritis in patients older than 18 years, one arthroplasty was excluded because of an outlier opioid dose, and a further 57% (85,724 of 150,574) were excluded because of our linkage criteria. Some of the linked arthroplasties could not be linked to a community pharmacy, leaving 28% (42,689 of 150,574) of THAs, which were performed between 2013 and 2018. For both TKA and THA, the mean age before surgery was 68 years, and roughly 60% of the population were women. We calculated the proportion of patients undergoing arthroplasties who had at least one opioid prescription in the year before arthroplasty and compared data from 2013 to 2018. Opioid prescription rates are given as defined daily dosages and morphine milligram equivalents (MMEs) per arthroplasty. Opioid prescriptions were assessed by preoperative quarter and by operation year. Possible changes over time in opioid exposure were investigated using linear regression, adjusted for age and gender, in which the month of operation since January 2013 was used as the determinant and MME as the outcome. This was done for all opioids combined and per opioid type. Possible changes in opioid prescription rates in the year before arthroplasty were assessed by comparing the time period of 1 to 3 months before surgery with the other quarters. Additionally, preoperative prescriptions per operation year were assessed per prescriber category: general practitioners, orthopaedic surgeons, rheumatologists, and others. All analyses were stratified by TKA or THA.
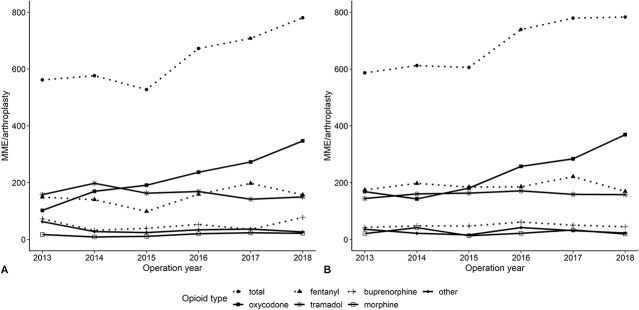
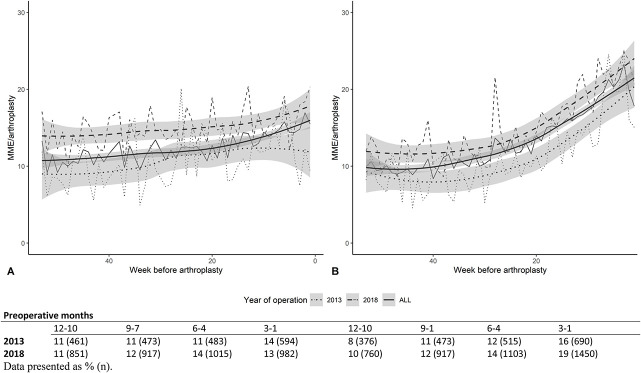
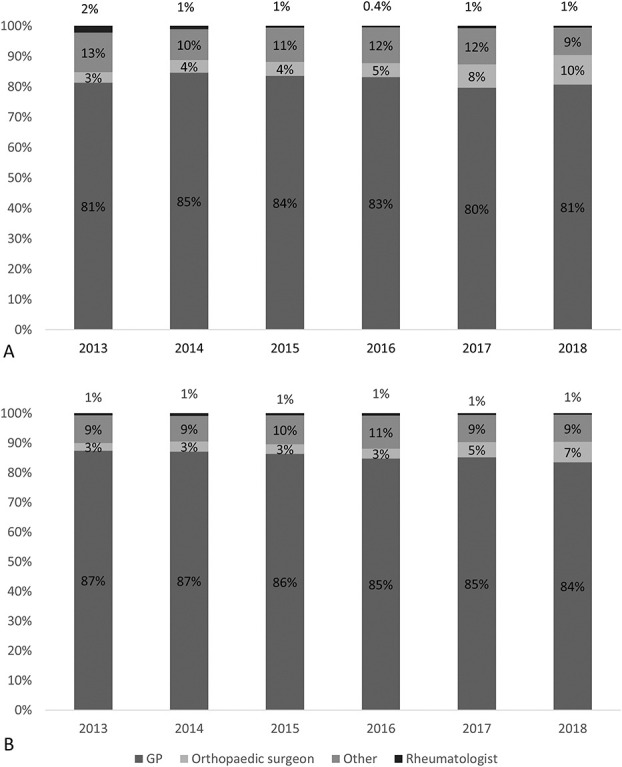
Results: The proportion of patients undergoing arthroplasties who had an opioid prescription before TKA increased from 25% (1079 of 4298) in 2013 to 28% (2097 of 7460) in 2018 (difference 3% [95% CI 1.35% to 4.65%]; p < 0.001), and before THA increased from 25% (1111 to 4451) to 30% (2323 to 7625) (difference 5% [95% CI 3.8% to 7.2%]; p < 0.001). The mean preoperative opioid prescription rate increased over time between 2013 and 2018 for both TKA and THA. For TKA, an adjusted monthly increase of 3.96 MME was observed (95% CI 1.8 to 6.1 MME; p < 0.001). For THA, the monthly increase was 3.8 MME (95% CI 1.5 to 6.0; p = 0.001. For both TKA and THA, there was a monthly increase in the preoperative oxycodone rate (3.8 MME [95% CI 2.5 to 5.1]; p < 0.001 and 3.6 [95% CI 2.6 to 4.7]; p < 0.001, respectively). For TKA, but not for THA, there was a monthly decrease in tramadol prescriptions (-0.6 MME [95% CI -1.0 to -0.2]; p = 0.006). Regarding the opioids prescribed in the year before surgery, there was a mean increase of 48 MME (95% CI 39.3 to 56.7 MME; p < 0.001) for TKA between 10 and 12 months and the last 3 months before surgery. For THA, this increase was 121 MME (95% CI 110 to 131 MME; p < 0.001). Regarding possible differences between 2013 and 2018, we only found differences in the period 10 to 12 months before TKA (mean difference 61 MME [95% CI 19.2 to 103.3]; p = 0.004) and the period 7 to 9 months before TKA (mean difference 66 MME [95% CI 22.0 to 110.9]; p = 0.003). For THA, there was an increase in the MMEs prescribed between 2013 and 2018 for all four quarters, with mean differences ranging from 43.9 to 55.4 MME (p < 0.05). The average proportion of preoperative opioid prescriptions prescribed by general practitioners ranged between 82% and 86% (41,037 of 49,855 for TKA and 49,137 of 57,289 for THA), between 4% and 6% (2924 of 49,855 for TKA and 2461 of 57,289 for THA), by orthopaedic surgeons, 1% by rheumatologists (409 of 49,855 for TKA and 370 of 57,289 for THA), and between 9% and 11% by other physicians (5485 of 49,855 for TKA and 5321 of 57,289 for THA). Prescriptions by orthopaedic surgeons increased over time, from 3% to 7% for THA (difference 4% [95% CI 3.6 to 4.9]) and 4% to 10% for TKA (difference 6% [95% CI 5% to 7%]; p < 0.001).
Conclusion: Between 2013 and 2018, preoperative opioid prescriptions increased in the Netherlands, mainly because of a shift to more oxycodone prescriptions. We also observed an increase in opioid prescriptions in the year before surgery. Although general practitioners were the main prescribers of preoperative oxycodone, prescriptions by orthopaedic surgeons also increased during the study period. Orthopaedic surgeons should address opioid use and its associated negative effects in preoperative consultations. More intradisciplinary collaboration seems important to limit the prescribing of preoperative opioids. Additionally, research is necessary to assess whether opioid cessation before surgery reduces the risk of adverse outcomes.
Level of evidence: Level III, therapeutic study.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: What Changes Have Occurred in Opioid Prescriptions and the Prescribers of Opioids Before TKA and THA? A Large National Registry Study.Clin Orthop Relat Res. 2023 Sep 1;481(9):1729-1731. doi: 10.1097/CORR.0000000000002733. Epub 2023 Jun 8. Clin Orthop Relat Res. 2023. PMID: 37288999 Free PMC article. No abstract available.
Similar articles
-
Out-of-hospital opioid prescriptions after knee and hip arthroplasty: prescribers and the first prescribed opioid.Br J Anaesth. 2023 Apr;130(4):459-467. doi: 10.1016/j.bja.2022.12.024. Epub 2023 Feb 28. Br J Anaesth. 2023. PMID: 36858887
-
The 2018 Chitranjan S. Ranawat, MD Award: Developing and Implementing a Novel Institutional Guideline Strategy Reduced Postoperative Opioid Prescribing After TKA and THA.Clin Orthop Relat Res. 2019 Jan;477(1):104-113. doi: 10.1007/s11999.0000000000000292. Clin Orthop Relat Res. 2019. PMID: 30794233 Free PMC article.
-
Opioid prescribing patterns after arthroplasty of the knee and hip: a Dutch nationwide cohort study from 2013 to 2018.Acta Orthop. 2022 Jul 15;93:667-681. doi: 10.2340/17453674.2022.3993. Acta Orthop. 2022. PMID: 35848731 Free PMC article.
-
Postoperative Opioid Consumption is Greater after Simultaneous versus Staged Bilateral Total Knee Arthroplasty.J Knee Surg. 2024 May;37(6):436-443. doi: 10.1055/s-0043-1775872. Epub 2023 Oct 18. J Knee Surg. 2024. PMID: 37852291 Review.
-
Opioid Consumption After Discharge From Total Knee and Hip Arthroplasty: A Systematic Review and Meta-Analysis.J Arthroplasty. 2024 Aug;39(8):2130-2136.e7. doi: 10.1016/j.arth.2024.01.063. Epub 2024 Feb 8. J Arthroplasty. 2024. PMID: 38336301
Cited by
-
Comparison of the Effects of Adductor Canal and Femoral Nerve Blocks on Postoperative Opioid Consumption and Inflammatory Factor Levels in Elderly Patients After Total Knee Arthroplasty: A Prospective Observational Study.J Pain Res. 2024 Jul 11;17:2375-2391. doi: 10.2147/JPR.S463097. eCollection 2024. J Pain Res. 2024. PMID: 39011277 Free PMC article.
-
Improved perioperative narcotic usage patterns in patients undergoing robotic-assisted compared to manual total hip arthroplasty.Arthroplasty. 2023 Nov 4;5(1):56. doi: 10.1186/s42836-023-00211-5. Arthroplasty. 2023. PMID: 37924164 Free PMC article.
References
-
- Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27:1578-1589. - PubMed
-
- Bedard NA, DeMik DE, Dowdle SB, Owens JM, Liu SS, Callaghan JJ. Does preoperative opioid use increase the risk of early revision total hip arthroplasty? J Arthroplasty. 2018;33:S154-S156. - PubMed
-
- Bedard NA, Demik DE, Dowdle SB, Owens JM, Liu SS, Callaghan JJ. Preoperative opioid use and its association with early revision of total knee arthroplasty. J Arthroplasty. 2018;33:3520-3523. - PubMed
-
- Blevins Peratikos M, Weeks HL, Pisansky AJB, Yong RJ, Stringer EA. Effect of preoperative opioid use on adverse outcomes, medical spending, and persistent opioid use following elective total joint arthroplasty in the United States: a large retrospective cohort study of administrative claims data. Pain Med. 2020;21:521-531. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
