

Thyroid-split tracheostomy: short- and long-term outcomes
- PMID: 37099433
- PMCID: PMC10132481
- DOI: 10.14639/0392-100X-N2192
Thyroid-split tracheostomy: short- and long-term outcomes
Abstract
Objective: Compare long-term outcomes of thyroid-split and standard thyroid-retraction tracheostomy in a large cohort.
Methods: The healthcare database of a university-affiliated hospital was searched for past patients over 18 years of age from all of the hospital's wards on whom an ear, nose, and throat specialist performed a tracheostomy in the operating room between 2010 and 2020. Clinical data were extracted from the hospital and outpatient medical records. Life-threatening and non-life-threatening intra-operative and early and late post-operative adverse events in patients who underwent split-thyroid tracheostomy were compared with those who underwent standard tracheostomy.
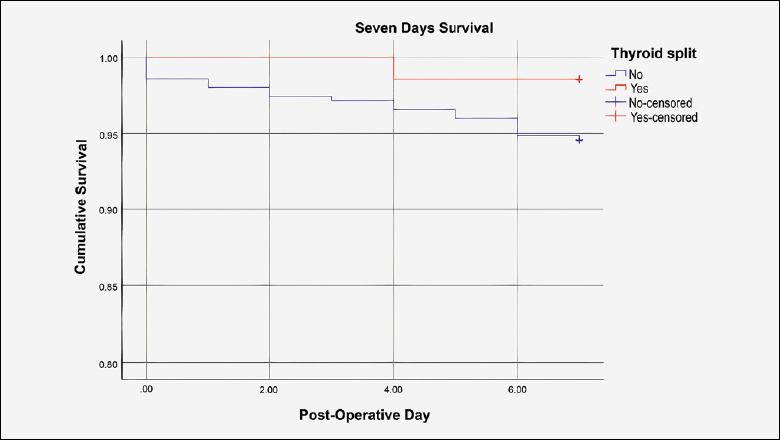
Results: There was no significant difference in intra-operative and early post-operative complications, hospitalisation length, or early reoperation and death rates between the 140 (28%) thyroid-split tracheostomy patients and the 354 (72%) standard tracheostomy patients, although the thyroid-split group had more non-decannulated patients and a longer operative time.
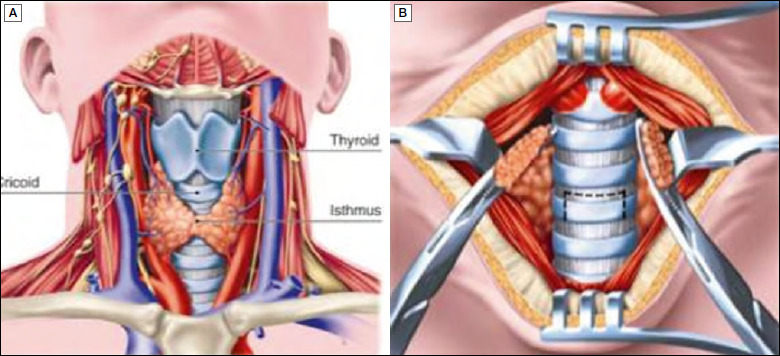
Conclusions: Thyroid-split tracheostomy is safe and feasible. Compared to the standard procedure, it provides better exposure and a similar rate of complications, although its de-cannulation success rate is lower.
Tracheotomia con istmectomia tiroidea: risultati a breve e lungo termine.
Obiettivo: Analisi delle complicanze in un’ampia coorte di pazienti sottoposti a tracheotomia chirurgica con e senza istmotomia tiroidea.
Metodi: Un apposito database retrospettivo è stato completato, includendo tutti i pazienti maggiorenni sottoposti a tracheotomia chirurgica presso il nostro ospedale universitario nel periodo tra il 2010 e il 2020. È stata condotta un’analisi comparativa degli eventi avversi precoci, tardivi, mortali e non, insorti tra i pazienti sottoposti a tracheotomia con e senza istmotomia tiroidea.
Risultati: Non è stata riscontrata alcuna differenza statisticamente significativa in merito a complicanze intra-operatorie, post-operatorie precoci e tardive, tempo di ospedalizzazione e tasso di decessi tra i 140 pazienti (28%) sottoposti a tracheotomia con istmotomia tiroidea e i 354 (72%) sottoposti a tracheostomia senza istmotomia. Nella prima coorte di pazienti sono stati riscontrati un tempo operatorio maggiore e un maggior tasso di pazienti non decannulati.
Conclusioni: La tracheotomia con istmotomia tiroidea si conferma una tecnica sicura. Se paragonata alla tracheotomia senza istmotomia, permette una esposizione migliore dell’asse tracheale e un tasso di complicanze sovrapponibile, nonostante il riscontro di un minore tasso di decannulazione.
Keywords: complications; decannulation; thyroid split; tracheostomy.
Copyright © 2023 Società Italiana di Otorinolaringoiatria e Chirurgia Cervico-Facciale, Rome, Italy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Johnson-Obaseki S, Veljkovic A, et al. Complication rates of open surgical versus percutaneous tracheostomy in critically ill patients. Laryngoscope 2016;126:2459-2467. https://doi.org/10.1002/lary.26019 10.1002/lary.26019 - DOI - PubMed
-
- Adly A, Youssef TA, El-Begermy MM, et al. Timing of tracheostomy in patients with prolonged endotracheal intubation: a systematic review. Eur Arch Otorhinolaryngol 2018;275:679-690. https://doi.org/10.1007/s00405-017-4838-7 10.1007/s00405-017-4838-7 - DOI - PubMed
-
- Wood DE. Tracheostomy. Chest Surg Clin N Am 1996;6:749-764. - PubMed
-
- Freeman BD, Kennedy C, Robertson TE, et al. Tracheostomy protocol: Experience with development and potential utility. Crit Care Med 2008;36:1742-1748. https://doi.org/10.1097/CCM.0b013e318174d9f6 10.1097/CCM.0b013e318174d9f6 - DOI - PubMed
-
- Cheung NH, Napolitano LM. Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care 2014;59:895-915; discussion 916-919. https://doi.org/10.4187/respcare.02971 10.4187/respcare.02971 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
