

Determining minimal clinically important differences in the North Star Ambulatory Assessment (NSAA) for patients with Duchenne muscular dystrophy
- PMID: 37099511
- PMCID: PMC10132589
- DOI: 10.1371/journal.pone.0283669
Determining minimal clinically important differences in the North Star Ambulatory Assessment (NSAA) for patients with Duchenne muscular dystrophy
Abstract
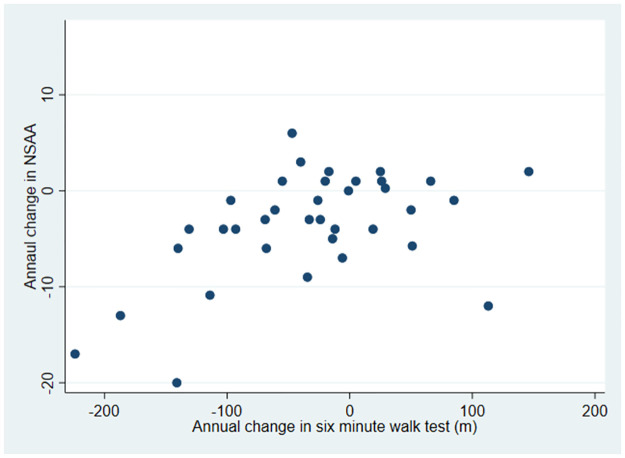
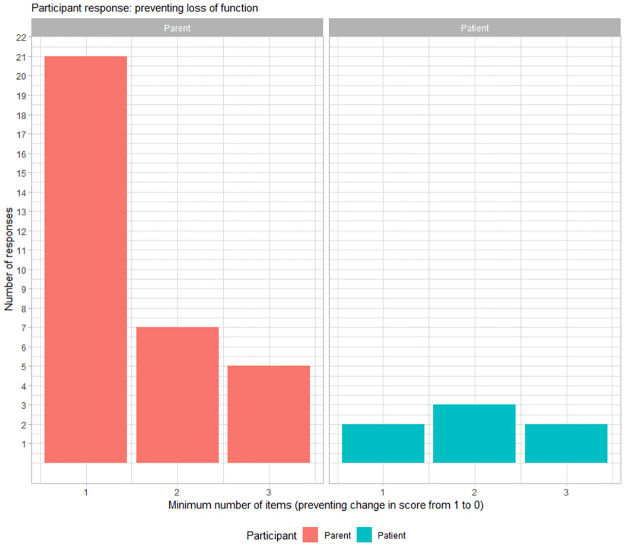
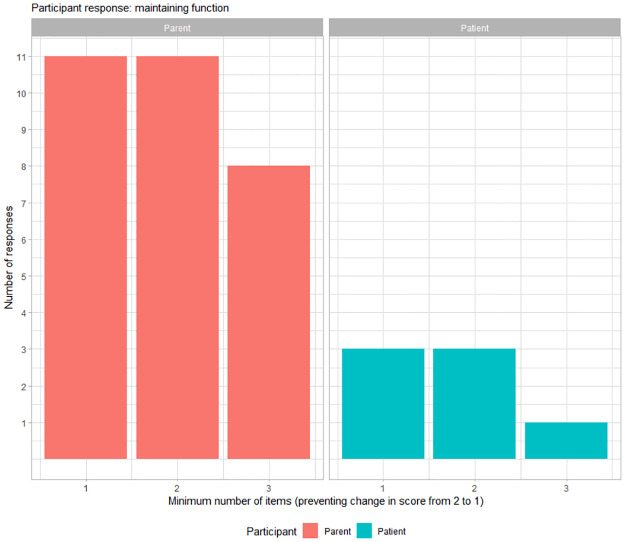
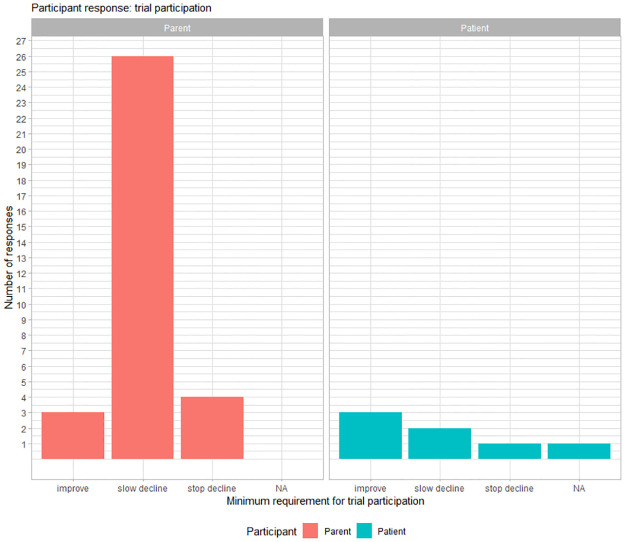
The North Star ambulatory assessment (NSAA) is a functional motor outcome measure in Duchenne muscular dystrophy (DMD), widely used in clinical trials and natural history studies, as well as in clinical practice. However, little has been reported on the minimal clinically important difference (MCID) of the NSAA. The lack of established MCID estimates for NSAA presents challenges in interpreting the significance of the results of this outcome measure in clinical trials, natural history studies and clinical practice. Combining statistical approaches and patient perspectives, this study estimated MCID for NSAA using distribution-based estimates of 1/3 standard deviation (SD) and standard error of measurement (SEM), an anchor-based approach, with six-minute walk distance (6MWD) as the anchor, and evaluation of patient and parent perception using participant-tailored questionnaires. The MCID for NSAA in boys with DMD aged 7 to 10 years based on 1/3 SD ranged from 2.3-2.9 points, and that on SEM ranged from 2.9-3.5 points. Anchored on the 6MWD, the MCID for NSAA was estimated as 3.5 points. When the impact on functional abilities was considered using participant response questionnaires, patients and parent perceived a complete loss of function in a single item or deterioration of function in one to two items of the assessment as an important change. Our study examines MCID estimates for total NSAA scores using multiple approaches, including the impact of patient and parent perspective on within scale changes in items based on complete loss of function and deterioration of function, and provides new insight on evaluation of differences in these widely used outcome measure in DMD.
Trial registration: ClinicalTrials.gov NCT02780492.
Copyright: © 2023 Ayyar Gupta et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
E.H.Niks report grants from Spieren voor Spieren, Duchenne Parent Project, ZonMW, AFM and PPMD. He has been site principal investigator for clinical trials conducted by BioMarin, GSK, Eli Lilly, Santhera Pharmaceuticals, Italfarmaco SpA, Roche Pharma, Reveragen, NS Pharma, Fibrogen, Sarepta, Alexion, Janssen and Argnx outside the submitted work. He also reports ad hoc consultancies for BioMarin, Summit, PTC therapeutics, WAVE Life Sciences, Edgewise, Epirium Bio, Janssen, Sarepta and Regenxbio. All reimbursements were received by the LUMC. No personal financial benefits were received. I.de Groot has received consulting and education fees from PTC Therapeutics, Santhera, Biomarin/Prosensa. J-Y.Hogrel has received consulting fees from Biogen, Sarepta, Minoryx and Roche. L.Servais has received consulting fees from Roche, Biogen, Avexis, Cytokinetics, Sarepta, Biomarin, Santhera, Servier, Biophytis and Dynacure. He is coordinating natural history studies funded by Valerion, Dynacure and Roche. A.Mayhew has received consulting fees from Roche, Novartis (Avexis), Biogen, Rehenxbio, PTC, BMS/Roche, Sarepta, Italfarmaco, Pfizer, Summit, Catabasis, Santhera, Vision, Mallinckrodt, Lysogen, Modis and Wave. V.Straub received speaker honoraria from Sanofi Genzyme and has participated in advisory boards for Audentes Therapeutics, Biogen, AveXis, Pharmaceuticals, Pfizer, Roche, Sanofi Genzyme, Sarepta Therapeutics, Summit Therapeutics and Wave Therapeutics. V.Ricotti is co-founder, EVP, CMO of DiNAQOR, and served as a consultant for Solid Biosciences and Antisense Therapeutics. F.Muntoni reports grants from Sarepta, grants from Wave, grants from PTC Therapeutics, personal fees from Avexis, Roche, Pfizer, Dyne Therapeutics, Sarepta, outside the submitted work. M.Chesshyre has had the costs associated with attending a conference (including travel, accommodation, conference fee, food and drink) funded by PTC Therapeutics. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Categorising trajectories and individual item changes of the North Star Ambulatory Assessment in patients with Duchenne muscular dystrophy.PLoS One. 2019 Sep 3;14(9):e0221097. doi: 10.1371/journal.pone.0221097. eCollection 2019. PLoS One. 2019. PMID: 31479456 Free PMC article.
-
Exploring the relationship between North Star Ambulatory Assessment and Health Utilities Index scores in Duchenne muscular dystrophy.Health Qual Life Outcomes. 2023 Jul 19;21(1):76. doi: 10.1186/s12955-023-02160-8. Health Qual Life Outcomes. 2023. PMID: 37468890 Free PMC article. Clinical Trial.
-
Quantifying Variability in Motor Function in Duchenne Muscular Dystrophy: UK Centiles for the NorthStar Ambulatory Assessment, 10 m Walk Run Velocity and Rise from Floor Velocity in GC Treated Boys.J Neuromuscul Dis. 2024;11(1):153-166. doi: 10.3233/JND-230159. J Neuromuscul Dis. 2024. PMID: 37980680 Free PMC article.
-
Efficacy and Safety of Vamorolone in Duchenne Muscular Dystrophy: A Systematic Review.Paediatr Drugs. 2024 Nov;26(6):695-707. doi: 10.1007/s40272-024-00655-5. Epub 2024 Sep 27. Paediatr Drugs. 2024. PMID: 39331339
-
Exon skipping for Duchenne muscular dystrophy: a systematic review and meta-analysis.Orphanet J Rare Dis. 2018 Jun 15;13(1):93. doi: 10.1186/s13023-018-0834-2. Orphanet J Rare Dis. 2018. PMID: 29907124 Free PMC article.
Cited by
-
"If you cannot measure it, you cannot improve it". Outcome measures in Duchenne Muscular Dystrophy: current and future perspectives.Acta Neurol Belg. 2025 Feb;125(1):1-12. doi: 10.1007/s13760-024-02600-2. Epub 2024 Jul 31. Acta Neurol Belg. 2025. PMID: 39080230 Free PMC article. Review.
-
A patient-centered qualitative evaluation of meaningful change on the NSAA and PUL in Duchenne Muscular Dystrophy.Front Neurol. 2025 Mar 4;16:1509174. doi: 10.3389/fneur.2025.1509174. eCollection 2025. Front Neurol. 2025. PMID: 40103935 Free PMC article.
-
Efficacy of delandistrogene moxeparvovec on Duchenne muscular dystrophy: a systematic review and meta-analysis.Hum Genet. 2025 Jun 26. doi: 10.1007/s00439-025-02758-6. Online ahead of print. Hum Genet. 2025. PMID: 40569438 Review. No abstract available.
-
Determining minimal clinically important differences in the Hammersmith Functional Motor Scale Expanded for untreated spinal muscular atrophy patients: An international study.Eur J Neurol. 2024 Aug;31(8):e16309. doi: 10.1111/ene.16309. Epub 2024 Apr 24. Eur J Neurol. 2024. PMID: 38656662 Free PMC article.
-
AAV gene therapy for Duchenne Muscular Dystrophy: lessons learned from a phase 3 trial.Gene Ther. 2024 Nov;31(11-12):541-543. doi: 10.1038/s41434-024-00494-6. Epub 2024 Oct 23. Gene Ther. 2024. PMID: 39443734 Review. No abstract available.
References
-
- McDonald CM, Campbell C, Torricelli RE, Finkel RS, Flanigan KM, Goemans N, et al.. Ataluren in patients with nonsense mutation Duchenne muscular dystrophy (ACT DMD): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017. Sep 23;390(10101):1489–1498. Epub 2017 Jul 17. doi: 10.1016/S0140-6736(17)31611-2 . - DOI - PubMed
-
- Charleston JS, Schnell FJ, Dworzak J, Donoghue C, Lewis S, Chen L, et al.. Eteplirsen treatment for Duchenne muscular dystrophy: Exon skipping and dystrophin production. Neurology. 2018. Jun 12;90(24): e2146–e2154. Epub 2018 May 11. Erratum in: Neurology. 2018 Sep 25;91(13):637. doi: 10.1212/WNL.0000000000005680 . - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
