The Burden of Human Bocavirus 1 in Hospitalized Children With Respiratory Tract Infections
- PMID: 37099765
- PMCID: PMC10231390
- DOI: 10.1093/jpids/piad027
The Burden of Human Bocavirus 1 in Hospitalized Children With Respiratory Tract Infections
Abstract
Background: Human bocavirus 1 (HBoV1) is frequently codetected with other viruses, and detected in asymptomatic children. Thus, the burden of HBoV1 respiratory tract infections (RTI) has been unknown. Using HBoV1-mRNA to indicate true HBoV1 RTI, we assessed the burden of HBoV1 in hospitalized children and the impact of viral codetections, compared with respiratory syncytial virus (RSV).
Methods: Over 11 years, we enrolled 4879 children <16 years old admitted with RTI. Nasopharyngeal aspirates were analyzed with polymerase chain reaction for HBoV1-DNA, HBoV1-mRNA, and 19 other pathogens.
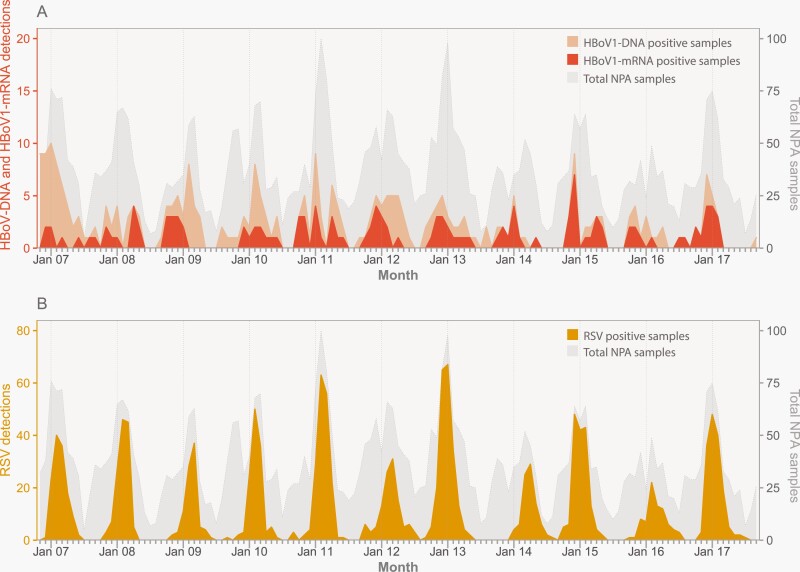
Results: HBoV1-mRNA was detected in 2.7% (130/4850) samples, modestly peaking in autumn and winter. Forty-three percent with HBoV1 mRNA were 12-17 months old, and only 5% were <6 months old. A total of 73.8% had viral codetections. It was more likely to detect HBoV1-mRNA if HBoV1-DNA was detected alone (odds ratio [OR]: 3.9, 95% confidence interval [CI]: 1.7-8.9) or with 1 viral codetection (OR: 1.9, 95% CI: 1.1-3.3), compared to ≥2 codetections. Codetection of severe viruses like RSV had lower odds for HBoV1-mRNA (OR: 0.34, 95% CI: 0.19-0.61). The yearly lower RTI hospitalization rate per 1000 children <5 years was 0.7 for HBoV1-mRNA and 8.7 for RSV.
Conclusions: True HBoV1 RTI is most likely when HBoV1-DNA is detected alone, or with 1 codetected virus. Hospitalization due to HBoV1 LRTI is 10-12 times less common than RSV.
Keywords: children; hospitalization rates; human bocavirus; respiratory tract infections; seasonality.
© The Author(s) 2023. Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society.
Figures