

Change in Platelet Count after Transjugular Intrahepatic Portosystemic Shunt Creation: An Advancing Liver Therapeutic Approaches (ALTA) Group Study
- PMID: 37100199
- PMCID: PMC10998695
- DOI: 10.1016/j.jvir.2023.04.015
Change in Platelet Count after Transjugular Intrahepatic Portosystemic Shunt Creation: An Advancing Liver Therapeutic Approaches (ALTA) Group Study
Abstract
Purpose: To evaluate recovery of platelet count after transjugular intrahepatic portosystemic shunt (TIPS) creation and patient factors predicting platelet recovery after TIPS creation.
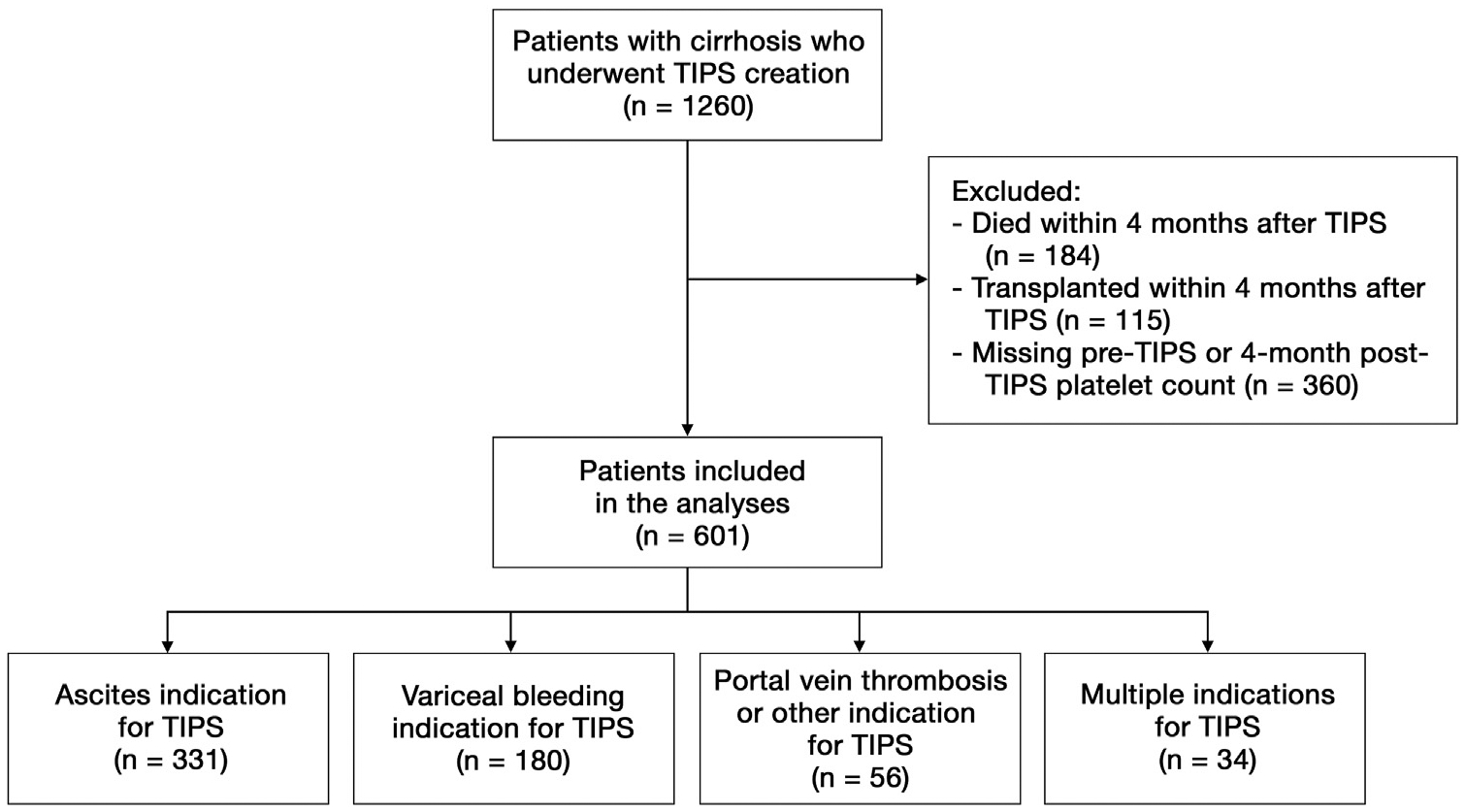
Materials and methods: Adults with cirrhosis who underwent TIPS creation at 9 U.S. hospitals from 2010 to 2015 were included in this retrospective analysis. Change in platelets from before TIPS to 4 months after TIPS creation was characterized. Logistic regression was used to assess factors associated with top quartile percentage platelet increase after TIPS. Subgroup analyses were performed among patients with a pre-TIPS platelet count of ≤50 ×109/L.
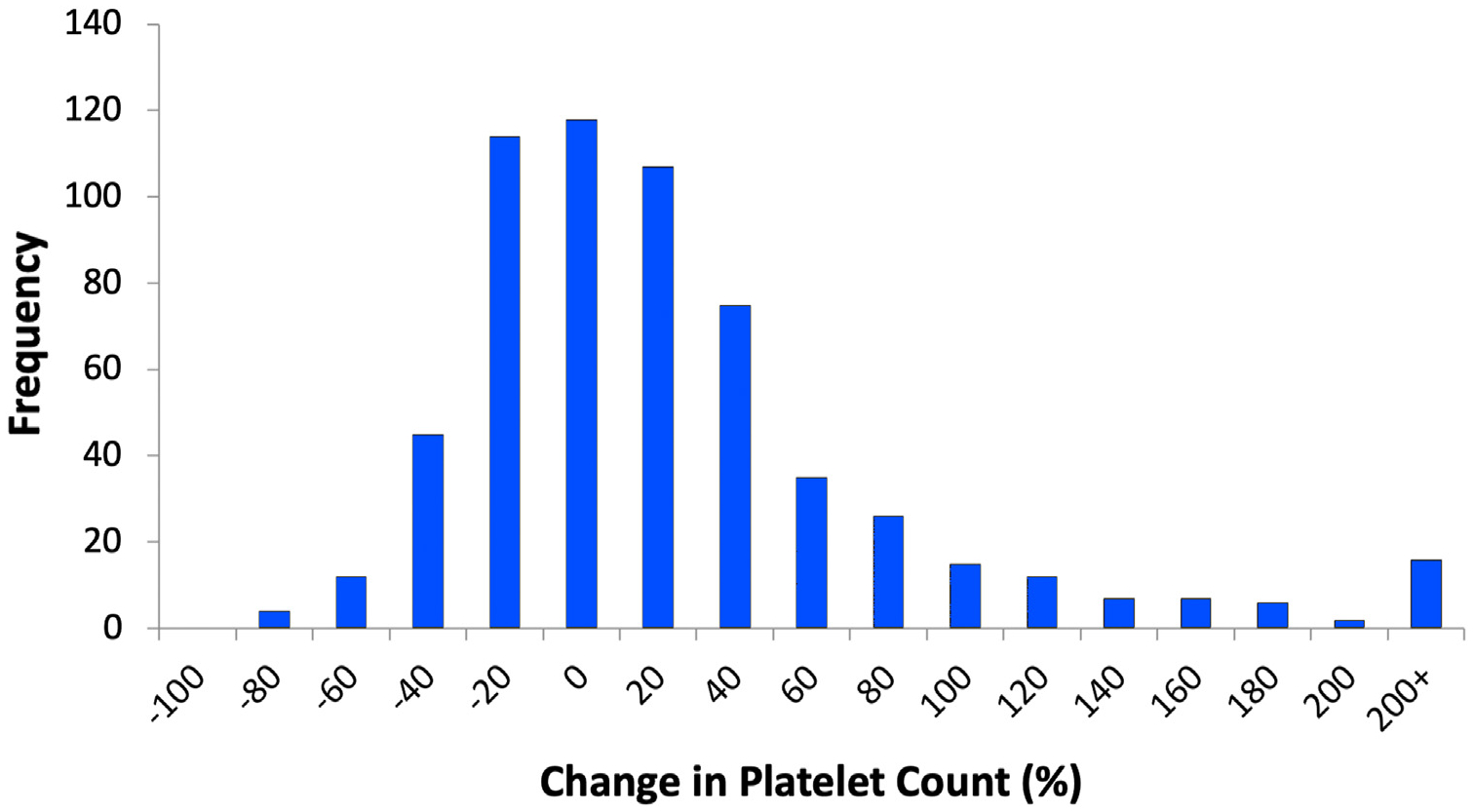
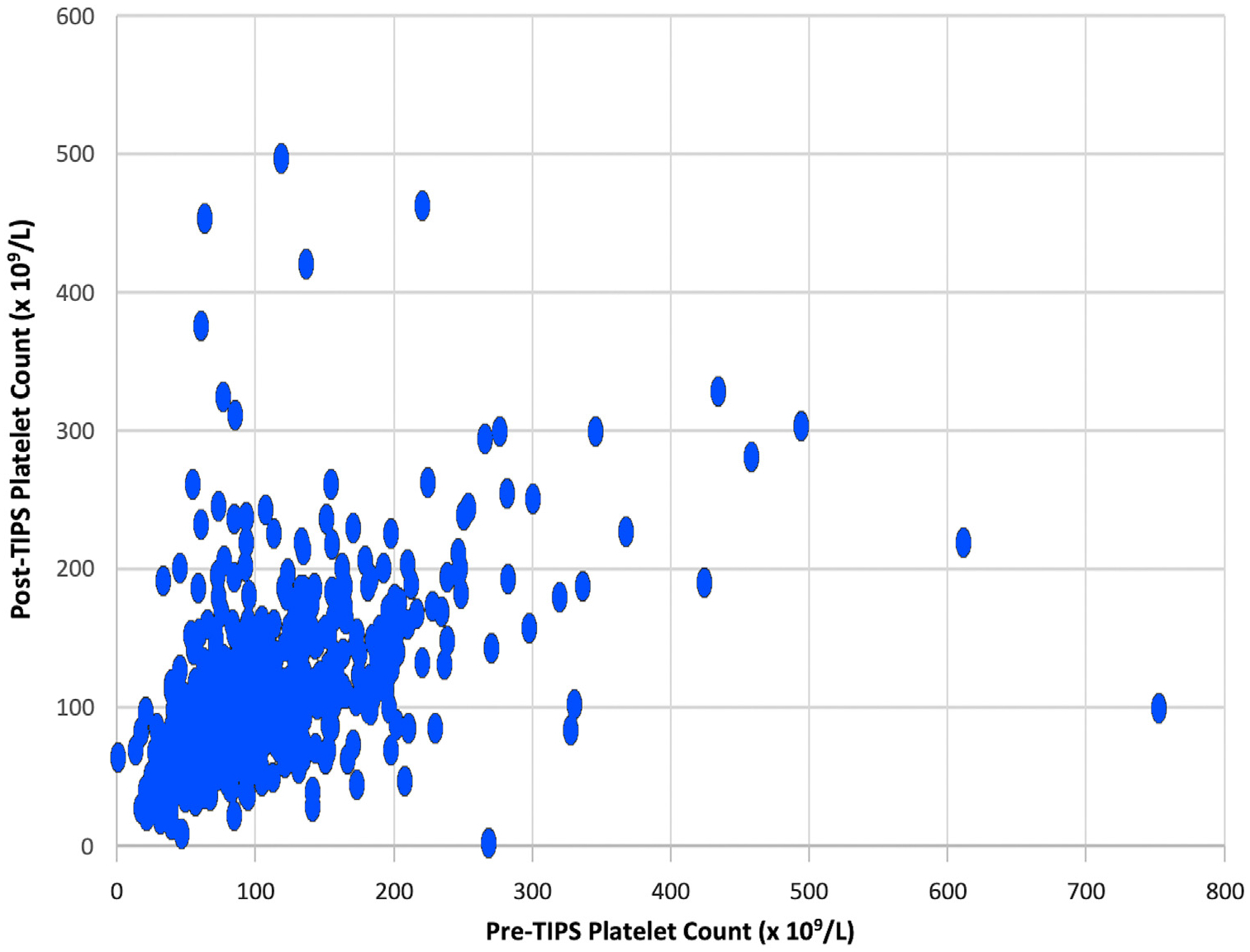
Results: A total of 601 patients were included. The median absolute change in platelets was 1 × 109/L (-26 × 109/L to 25 × 109/L). Patients with top quartile percent platelet increase experienced ≥32% platelet increase. In multivariable analysis, pre-TIPS platelet counts (odds ratio [OR], 0.97 per 109/L; 95% CI, 0.97-0.98), age (OR, 1.24 per 5 years; 95% CI, 1.10-1.39), and pre-TIPS model for end-stage liver disease (MELD) scores (OR, 1.06 per point; 95% CI, 1.02-1.09) were associated with top quartile (≥32%) platelet increase. Ninety-four (16%) patients had a platelet count of ≤50 × 109/L before TIPS. The median absolute platelet change was 14 × 109/L (2 × 109/L to 34 × 109/L). Fifty-four percent of patients in this subgroup were in the top quartile for platelet increase. In multivariable logistic regression, age (OR, 1.50 per 5 years; 95% CI, 1.11-2.02) was the only factor associated with top quartile platelet increase in this subgroup.
Conclusions: TIPS creation did not result in significant platelet increase, except among patients with a platelet count of ≤50 × 109/L before TIPS. Lower pre-TIPS platelet counts, older age, and higher pre-TIPS MELD scores were associated with top quartile (≥32%) platelet increase in the entire cohort, whereas only older age was associated with this outcome in the patient subset with a pre-TIPS platelet count of ≤50 × 109/L.
Copyright © 2023. Published by Elsevier Inc.
Figures
Comment in
-
Platelet Count after Transjugular Intrahepatic Portosystemic Shunt: Response to Wong et al, JVIR, August 2023.J Vasc Interv Radiol. 2024 Mar;35(3):469. doi: 10.1016/j.jvir.2023.11.022. Epub 2023 Dec 1. J Vasc Interv Radiol. 2024. PMID: 38043706 No abstract available.
Similar articles
-
Early Liver Failure after Transjugular Intrahepatic Portosystemic Shunt in Patients with Cirrhosis with Model for End-Stage Liver Disease Score of 12 or Less: Incidence, Outcome, and Prognostic Factors.Radiology. 2016 Aug;280(2):622-9. doi: 10.1148/radiol.2016151625. Epub 2016 Mar 14. Radiology. 2016. PMID: 26982564
-
Socioeconomic Status Is Associated with the Risk of Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt Creation.J Vasc Interv Radiol. 2021 Jul;32(7):950-960.e1. doi: 10.1016/j.jvir.2020.11.022. Epub 2021 Mar 2. J Vasc Interv Radiol. 2021. PMID: 33663923
-
MELD 3.0 Score for Predicting Survival in Patients with Cirrhosis After Transjugular Intrahepatic Portosystemic Shunt Creation.Dig Dis Sci. 2023 Jul;68(7):3185-3192. doi: 10.1007/s10620-023-07834-3. Epub 2023 Jan 30. Dig Dis Sci. 2023. PMID: 36715817
-
Psoas Muscle Density in Combination with Model for End-Stage Liver Disease Score Can Improve Survival Predictability in Transjugular Intrahepatic Portosystemic Shunts.J Vasc Interv Radiol. 2019 Feb;30(2):154-161. doi: 10.1016/j.jvir.2018.10.006. J Vasc Interv Radiol. 2019. PMID: 30717946
-
Surgical portosystemic shunts versus transjugular intrahepatic portosystemic shunt for variceal haemorrhage in people with cirrhosis.Cochrane Database Syst Rev. 2018 Oct 31;10(10):CD001023. doi: 10.1002/14651858.CD001023.pub3. Cochrane Database Syst Rev. 2018. PMID: 30378107 Free PMC article.
References
-
- LaBerge JM. Transjugular intrahepatic portosystemic shunt—role in treating intractable variceal bleeding, ascites, and hepatic hydrothorax. Clin Liver Dis 2006; 10:583–598, ix. - PubMed
-
- Caldwell SH, Hoffman M, Lisman T, et al. Coagulation disorders and hemostasis in liver disease: pathophysiology and critical assessment of current management. Hepatology 2006; 44:1039–1046. - PubMed
-
- Northup PG, Garcia-Pagan JC, Garcia-Tsao G, et al. Vascular liver disorders, portal vein thrombosis, and procedural bleeding in patients with liver disease: 2020 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2021; 73:366–413. - PubMed
