

Aerosol pulmonary immune engineering
- PMID: 37100206
- PMCID: PMC10527166
- DOI: 10.1016/j.addr.2023.114831
Aerosol pulmonary immune engineering
Abstract
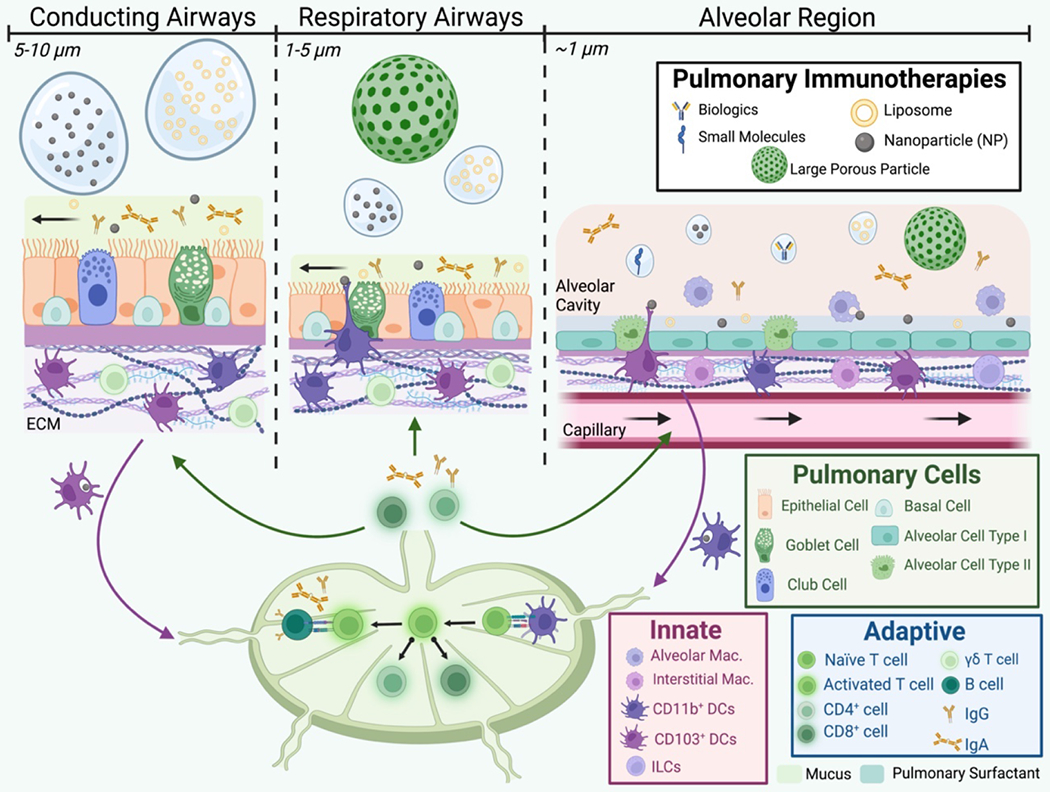
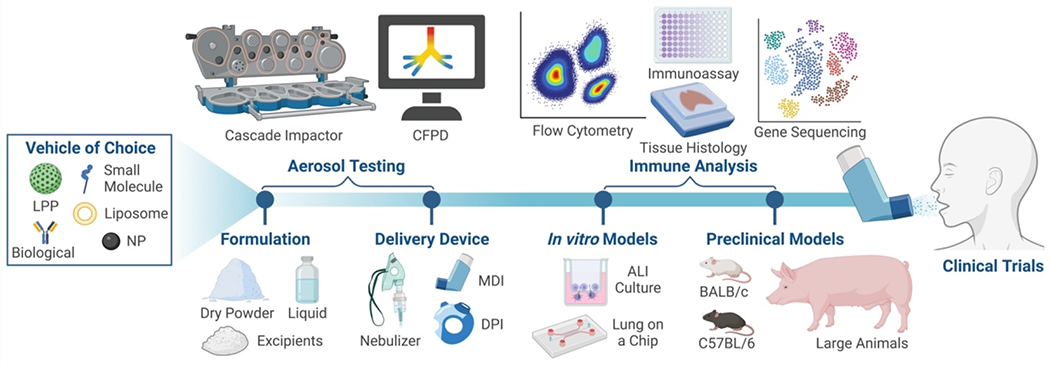
Aerosolization of immunotherapies poses incredible potential for manipulating the local mucosal-specific microenvironment, engaging specialized pulmonary cellular defenders, and accessing mucosal associated lymphoid tissue to redirect systemic adaptive and memory responses. In this review, we breakdown key inhalable immunoengineering strategies for chronic, genetic, and infection-based inflammatory pulmonary disorders, encompassing the historic use of immunomodulatory agents, the transition to biological inspired or derived treatments, and novel approaches of complexing these materials into drug delivery vehicles for enhanced release outcomes. Alongside a brief description of key immune targets, fundamentals of aerosol drug delivery, and preclinical pulmonary models for immune response, we survey recent advances of inhaled immunotherapy platforms, ranging from small molecules and biologics to particulates and cell therapies, as well as prophylactic vaccines. In each section, we address the formulation design constraints for aerosol delivery as well as advantages for each platform in driving desirable immune modifications. Finally, prospects of clinical translation and outlook for inhaled immune engineering are discussed.
Keywords: Asthma; Biologics; COPD; COVID-19; Cancer; Cystic fibrosis; Immune engineering; Immunotherapy; Particulates; Pulmonary delivery; Small molecules.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Pharmaceutical aerosols for the treatment and prevention of tuberculosis.Front Cell Infect Microbiol. 2012 Sep 7;2:118. doi: 10.3389/fcimb.2012.00118. eCollection 2012. Front Cell Infect Microbiol. 2012. PMID: 22973562 Free PMC article. Review.
-
Advanced therapeutic inhalation aerosols of a Nrf2 activator and RhoA/Rho kinase (ROCK) inhibitor for targeted pulmonary drug delivery in pulmonary hypertension: design, characterization, aerosolization, in vitro 2D/3D human lung cell cultures, and in vivo efficacy.Ther Adv Respir Dis. 2021 Jan-Dec;15:1753466621998245. doi: 10.1177/1753466621998245. Ther Adv Respir Dis. 2021. PMID: 33719747 Free PMC article.
-
Engineering drug delivery systems to overcome mucosal barriers for immunotherapy and vaccination.Tissue Barriers. 2020;8(1):1695476. doi: 10.1080/21688370.2019.1695476. Epub 2019 Nov 28. Tissue Barriers. 2020. PMID: 31775577 Free PMC article.
-
Dry powder inhalers in COPD, lung inflammation and pulmonary infections.Expert Opin Drug Deliv. 2015 Jun;12(6):947-62. doi: 10.1517/17425247.2015.977783. Epub 2014 Nov 12. Expert Opin Drug Deliv. 2015. PMID: 25388926 Review.
Cited by
-
Secretome of EMSCs neutralizes LPS‑induced acute lung injury via aerosol administration.Int J Mol Med. 2023 Nov;52(5):104. doi: 10.3892/ijmm.2023.5307. Epub 2023 Sep 29. Int J Mol Med. 2023. PMID: 37772372 Free PMC article.
-
New insights for the development of efficient DNA vaccines.Microb Biotechnol. 2024 Nov;17(11):e70053. doi: 10.1111/1751-7915.70053. Microb Biotechnol. 2024. PMID: 39545748 Free PMC article. Review.
-
Recent Developments in Aerosol Pulmonary Drug Delivery: New Technologies, New Cargos, and New Targets.Annu Rev Biomed Eng. 2024 Jul;26(1):307-330. doi: 10.1146/annurev-bioeng-110122-010848. Epub 2024 Jun 20. Annu Rev Biomed Eng. 2024. PMID: 38424089 Free PMC article. Review.
-
Hydrogen-induced disruption of the airway mucus barrier enhances nebulized RNA delivery to reverse pulmonary fibrosis.Sci Adv. 2025 Apr 18;11(16):eadt2752. doi: 10.1126/sciadv.adt2752. Epub 2025 Apr 16. Sci Adv. 2025. PMID: 40238879 Free PMC article.
-
Inhaled biologics for respiratory diseases: clinical potential and emerging technologies.Drug Deliv Transl Res. 2025 Jul 14. doi: 10.1007/s13346-025-01909-6. Online ahead of print. Drug Deliv Transl Res. 2025. PMID: 40660066
References
-
- Anderson S, Atkins P, Bäckman P, Cipolla D, Clark A, Daviskas E, Disse B, Entcheva-Dimitrov P, Fuller R, Gonda I, Lundbäck H, Olsson B, Weers J, Inhaled Medicines: Past, Present, and Future, Pharmacological Reviews, 74 (2022) 48. - PubMed
-
• Excellent recent perspective of the state of inhaled medicines
-
- Katrivesis K, Elia J, Etiz B, Cooley-Rieders K, Hosseinian S, Melucci S, An Overview of Lung Anatomy and Physiology, in: Hakimi AA, Milner TE, Rajan GR, Wong BJF (Eds.) Mechanical Ventilation Amid the COVID-19 Pandemic: A Guide for Physicians and Engineers, Springer International Publishing, Cham, 2022, pp. 5–24.
-
- West JB, Luks A, West’s Respiratory Physiology: The Essentials, Wolters Kluwer; 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
