

Health Status and Clinical Outcomes in Older Adults With Chronic Coronary Disease: The ISCHEMIA Trial
- PMID: 37100486
- PMCID: PMC10902923
- DOI: 10.1016/j.jacc.2023.02.048
Health Status and Clinical Outcomes in Older Adults With Chronic Coronary Disease: The ISCHEMIA Trial
Abstract
Background: Whether initial invasive management in older vs younger adults with chronic coronary disease and moderate or severe ischemia improves health status or clinical outcomes is unknown.
Objectives: The goal of this study was to examine the impact of age on health status and clinical outcomes with invasive vs conservative management in the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial.
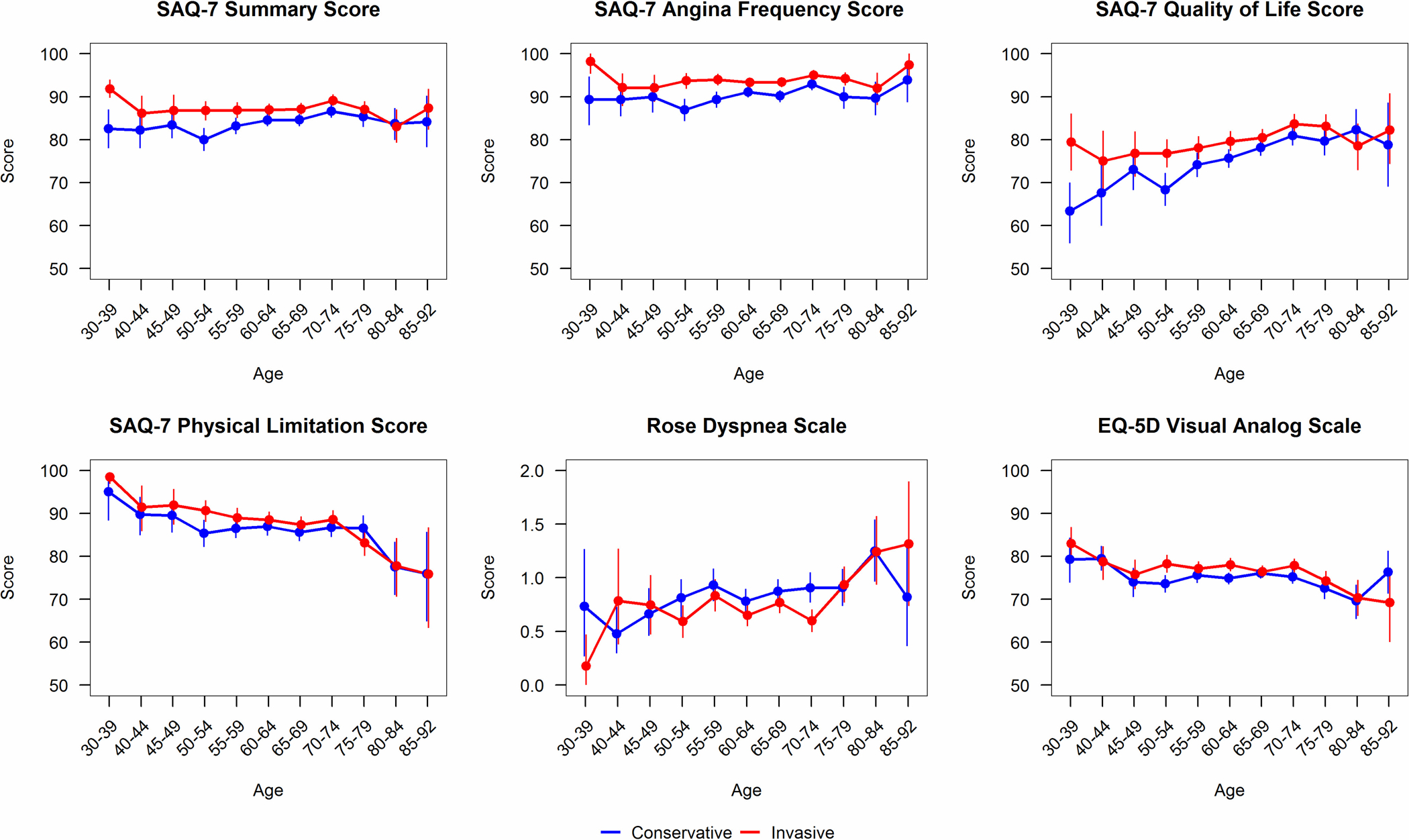
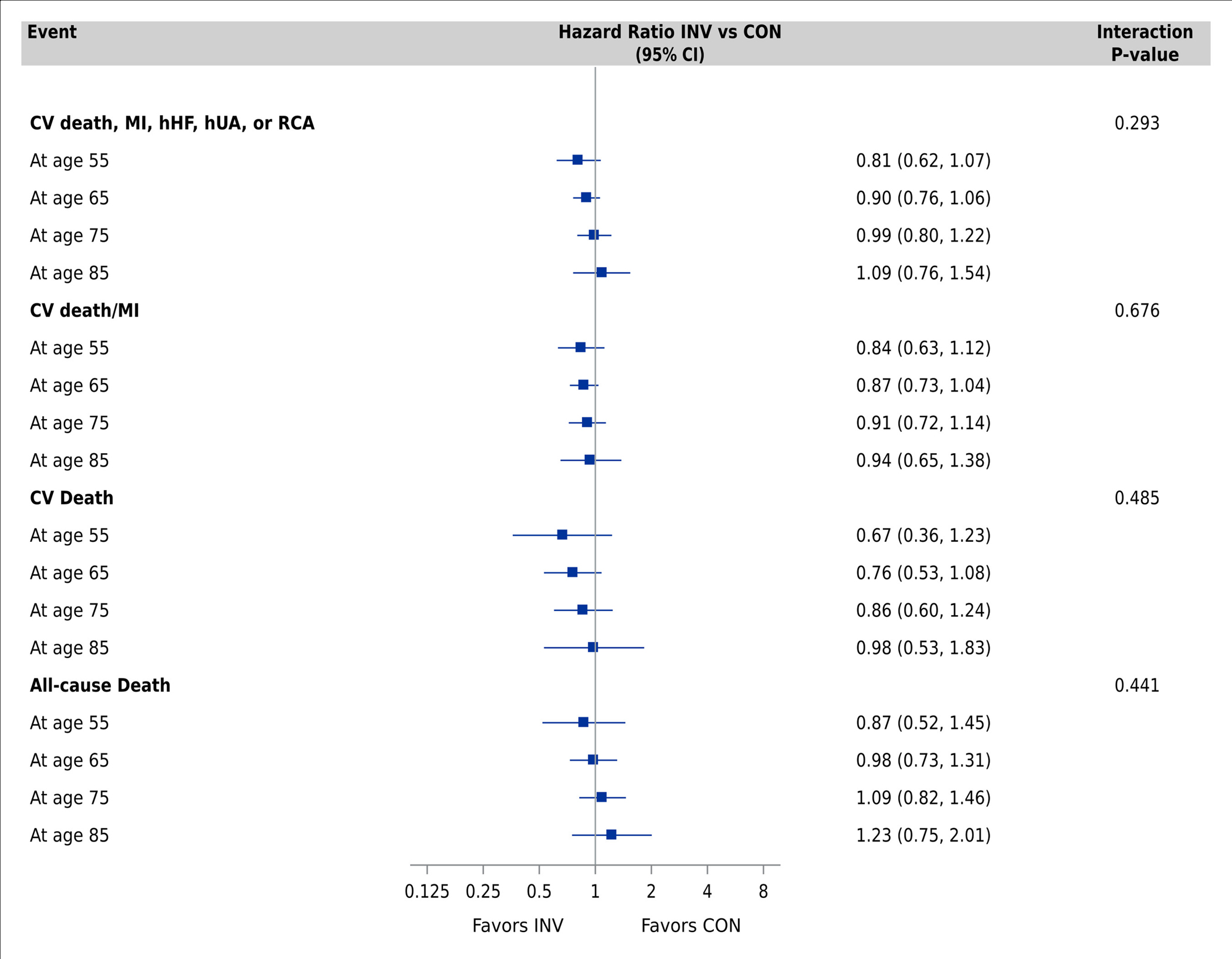
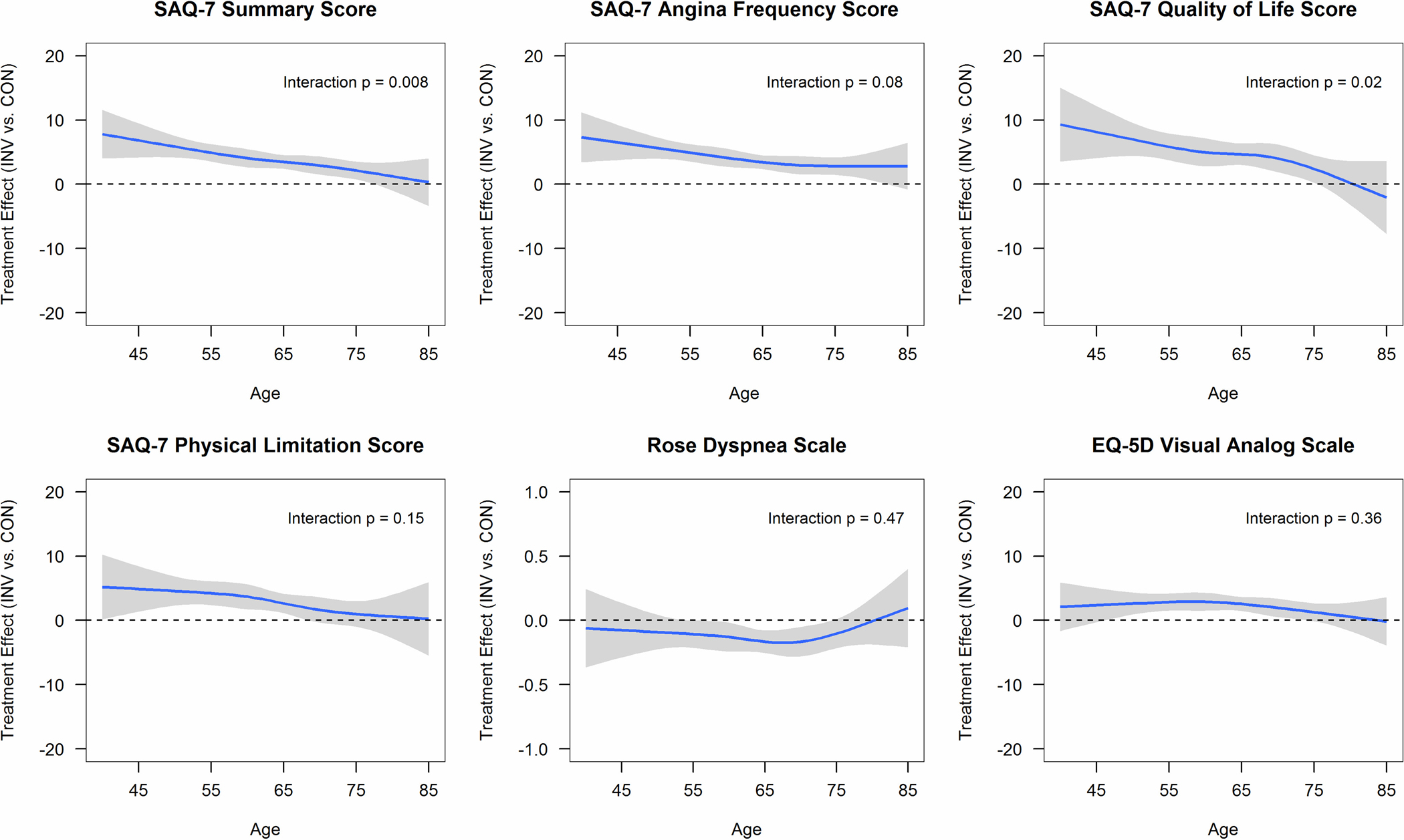
Methods: One-year angina-specific health status was assessed with the 7-item Seattle Angina Questionnaire (SAQ) (score range 0-100; higher scores indicate better health status). Cox proportional hazards models estimated the treatment effect of invasive vs conservative management as a function of age on the composite clinical outcome of cardiovascular death, myocardial infarction, or hospitalization for resuscitated cardiac arrest, unstable angina, or heart failure.
Results: Among 4,617 participants, 2,239 (48.5%) were aged <65 years, 1,713 (37.1%) were aged 65 to 74 years, and 665 (14.4%) were aged ≥75 years. Baseline SAQ summary scores were lower in participants aged <65 years. Fully adjusted differences in 1-year SAQ summary scores (invasive minus conservative) were 4.90 (95% CI: 3.56-6.24) at age 55 years, 3.48 (95% CI: 2.40-4.57) at age 65 years, and 2.13 (95% CI: 0.75-3.51) at age 75 years (Pinteraction = 0.008). Improvement in SAQ Angina Frequency was less dependent on age (Pinteraction = 0.08). There were no age differences between invasive vs conservative management on the composite clinical outcome (Pinteraction = 0.29).
Conclusions: Older patients with chronic coronary disease and moderate or severe ischemia had consistent improvement in angina frequency but less improvement in angina-related health status with invasive management compared with younger patients. Invasive management was not associated with improved clinical outcomes in older or younger patients. (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches [ISCHEMIA]; NCT01471522).
Keywords: coronary artery disease; older adults; quality of life.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This project was supported in part by National Institutes of Health grants U01HL105907, U01HL105462, U01HL105561, and U01HL105565; and in part by Clinical Translational Science Award numbers 11UL1 TR001445 and UL1 TR002243 from the National Center for Advancing Translational Sciences. The contents of this project are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences; the National Heart, Lung, and Blood Institute; the National Institutes of Health; or the Department of Health and Human Services. Dr Nguyen is currently supported by the National Heart, Lung, and Blood Institute under Award Number T32HL110837. Dr Spertus has received grants from the National Heart, Lung, and Blood Institute during the conduct of the study; has received personal fees from Bayer, Novartis, AstraZeneca, Amgen, Janssen, and United Healthcare; has received grants from the American College of Cardiology, outside the submitted work; has a patent copyright to SAQ with royalties paid; is on the Board of Directors for Blue Cross Blue Shield of Kansas City; and has equity in Health Outcomes Sciences. Dr Newman, Dr Alexander, Mrs Stevens, Dr O'Brien, Dr Gamma, Dr Perna, Dr Garg, Dr Vertes, Dr Smanio, Dr Senior, Dr Held, and Dr Maron have received grants from the National Heart, Lung, and Blood Institute during the conduct of the study. Mr Jones reports employment by the National Heart, Lung, and Blood Institute during the conduct of the study. Dr Chow holds the Saul and Edna Goldfarb Chair in Cardiac Imaging Research; receives research support from TD Bank, CV Diagnostix, AusculSciences, and Siemens Healthineers; and has equity interest in General Electric. Dr White has received grants from the National Heart, Lung, and Blood Institute during the conduct of the study; has received grant support paid to the institution and fees for serving on a steering committee for the ODYSSEY OUTCOMES trial from Sanofi and Regeneron Pharmaceuticals, for the ACCELERATE study from Eli Lilly, for the STRENGTH trial from Omthera Pharmaceuticals, for the HEART-FID study from American Regent, for the CAMELLIA-TIMI study from Eisai Inc, for the dal-GenE study from DalCor Pharma UK Inc, for the AEGIS-II study from CSL Behring, for the SCORED trial and the SOLOIST-WHF trial from Sanofi Australia Pty Ltd, and for the CLEAR Outcomes Study from Esperion Therapeutics Inc. Dr White was on the Advisory Board for Genentech, Inc; and has received lecture fees from AstraZeneca. Dr Boden has received grants from the National Heart, Lung, and Blood Institute during the conduct of the study; has received grants from AbbVie, Amarin, and Amgen; and has received personal fees from Amgen, the Cleveland Clinic Clinical Coordinating Center, and Janssen, outside the submitted work. Dr Mark has received grants from the National Heart, Lung, and Blood Institute during the conduct of the study; and has received grants from HeartFlow and Merck, outside the submitted work. Dr Reynolds has received funding for this research from the National Heart, Lung, and Blood Institute; and has received in-kind donations for unrelated research from Abbott Vascular, Siemens, and Philips. Dr Bangalore has received grants from the National Heart, Lung, and Blood Institute and Abbott Vascular; and serves on the advisory board for Abbott Vascular, Pfizer, Amgen, Biotronik, Meril, and Reata. Dr Chan has received funding from the American Heart Association; and is a consultant for Optum Rx. Dr Stone has received grants and personal fees from the National Heart, Lung, and Blood Institute during the conduct of the study; has received personal fees from Terumo, Amaranth, Shockwave, TherOx, Reva, Vascular Dynamics, Robocath, HeartFlow, Gore, Ablative Solutions, Matrizyme, Miracor, Neovasc, V-Wave, Abiomed, Claret, Sirtex, MAIA Pharmaceuticals, and Vectorious; has received personal fees and has equity/options from VALFIX, Ancora, Qool Therapeutics, SpectraWave, and Orchestra Biomed; has equity/options from Cagent, Applied Therapeutics, BioStar family of funds, MedFocus family of funds, and Aria; and has equity/options from Cardiac Success, outside the submitted work. Dr Hochman is Principal Investigator for the ISCHEMIA trial for which, in addition to support by a National Heart, Lung, and Blood Institute grant, devices and medications were provided by Abbott Vascular, Medtronic, Inc, Abbott Laboratories (formerly St Jude Medical, Inc), Royal Philips NV (formerly Volcano Corporation), Arbor Pharmaceuticals, LLC, AstraZeneca Pharmaceuticals, LP, Merck Sharp & Dohme Corp, Omron Healthcare, Inc, Sunovion Pharmaceuticals, Inc, Espero BioPharma, and Amgen, Inc, as well as financial donations from Arbor Pharmaceuticals LLC and AstraZeneca Pharmaceuticals LP. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Stable Coronary Artery Disease in the Age of Geriatric Cardiology.J Am Coll Cardiol. 2023 May 2;81(17):1710-1713. doi: 10.1016/j.jacc.2023.03.378. J Am Coll Cardiol. 2023. PMID: 37100487 Free PMC article. No abstract available.
References
-
- Tegn N, Eek C, Abdelnoor M, et al. Patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris randomised to an invasive versus conservative strategy: angiographic and procedural results from the After Eighty study. Open Hear. 2020;7(2):e001256. doi: 10.1136/openhrt-2020-001256 - DOI - PMC - PubMed
-
- Tsai TT, Patel UD, Chang TI, et al. Validated contemporary risk model of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the National Cardiovascular Data Registry Cath-PCI Registry. J Am Heart Assoc. 2014;3(6):e001380. doi: 10.1161/JAHA.114.001380 - DOI - PMC - PubMed
-
- Rao SV, McCoy LA, Spertus JA, et al. An updated bleeding model to predict the risk of post-procedure bleeding among patients undergoing percutaneous coronary intervention: a report using an expanded bleeding definition from the National Cardiovascular Data Registry CathPCI Registry. JACC Cardiovasc Interv. 2013;6(9):897–904. doi: 10.1016/j.jcin.2013.04.016 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
