

Clinico-imaging features of subjects at risk of Lewy body disease in NaT-PROBE baseline analysis
- PMID: 37100802
- PMCID: PMC10133289
- DOI: 10.1038/s41531-023-00507-y
Clinico-imaging features of subjects at risk of Lewy body disease in NaT-PROBE baseline analysis
Abstract
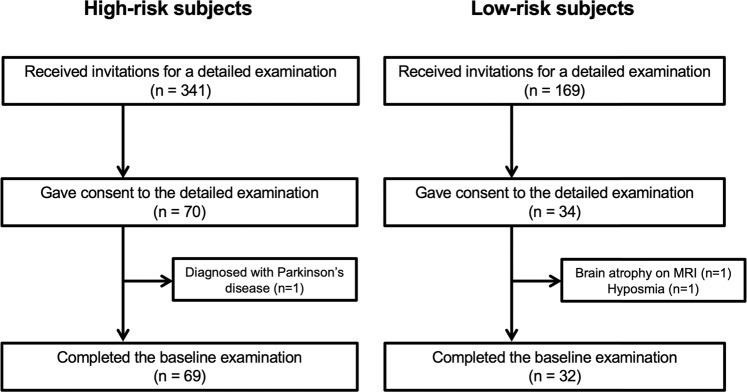
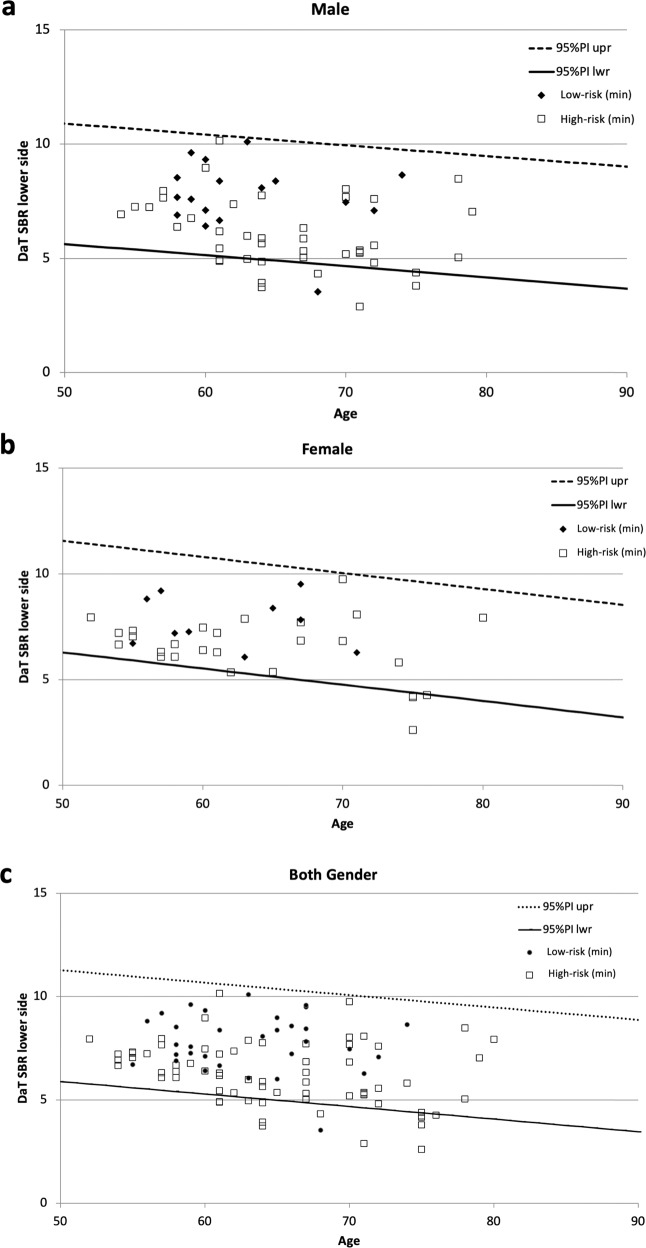
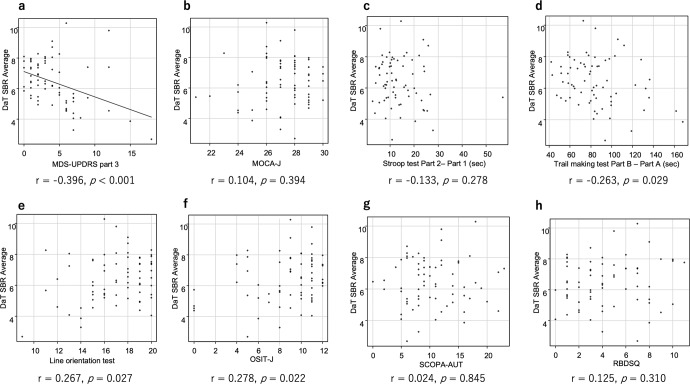
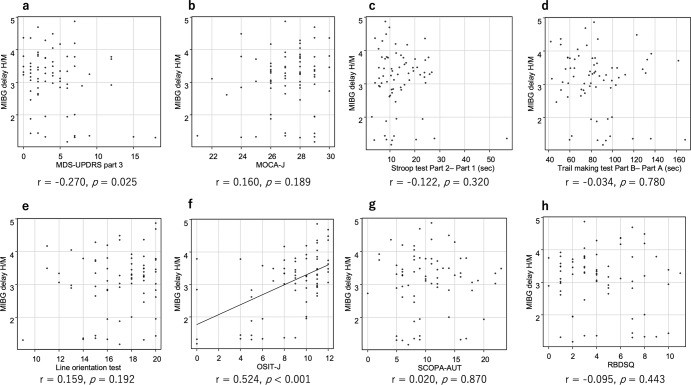
Individuals with prodromal symptoms of Lewy body disease (LBD), such as rapid eye movement sleep behavior disorder (RBD), often showed imaging defects similar to patients with Parkinson's disease and dementia with Lewy bodies. We examined dopamine transporter (DaT) single-photon-emission computed tomography (SPECT) and metaiodobenzylguanidine (MIBG) scintigraphy in 69 high-risk subjects with ≥2 prodromal symptoms (dysautonomia, hyposmia, and probable RBD) and 32 low-risk subjects without prodromal symptoms, whom were identified through a questionnaire survey of health checkup examinees. The high-risk subjects had significantly worse scores on Stroop test, line orientation test, and the Odor Stick Identification Test for Japanese than the low-risk subjects. The prevalence of abnormalities on DaT-SPECT was higher in the high-risk group than in the low-risk group (24.6% vs. 6.3%, p = 0.030). A decreased uptake on DaT-SPECT was associated with motor impairment, and MIBG scintigraphy defects were associated with hyposmia. The simultaneous evaluation of DaT-SPECT and MIBG scintigraphy may capture a wide range of individuals with prodromal LBD.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Grants and funding
- JP20dm0107155/Japan Agency for Medical Research and Development (AMED)
- JP22dk0207052/Japan Agency for Medical Research and Development (AMED)
- JP22ae0101077/Japan Agency for Medical Research and Development (AMED)
- JP22lk0201124/Japan Agency for Medical Research and Development (AMED)
- JP21K19443/MEXT | Japan Society for the Promotion of Science (JSPS)
LinkOut - more resources
Full Text Sources
