

Treating intrusive memories after trauma in healthcare workers: a Bayesian adaptive randomised trial developing an imagery-competing task intervention
- PMID: 37100869
- PMCID: PMC10131522
- DOI: 10.1038/s41380-023-02062-7
Treating intrusive memories after trauma in healthcare workers: a Bayesian adaptive randomised trial developing an imagery-competing task intervention
Abstract
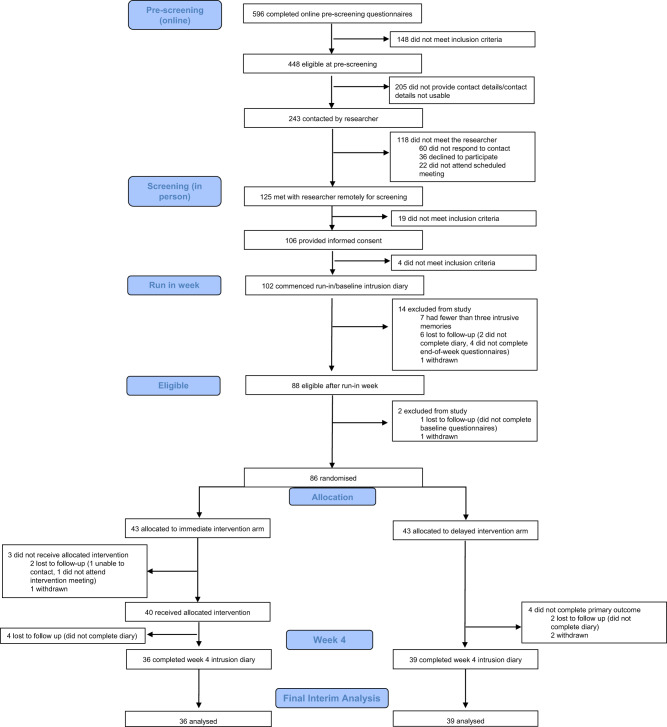
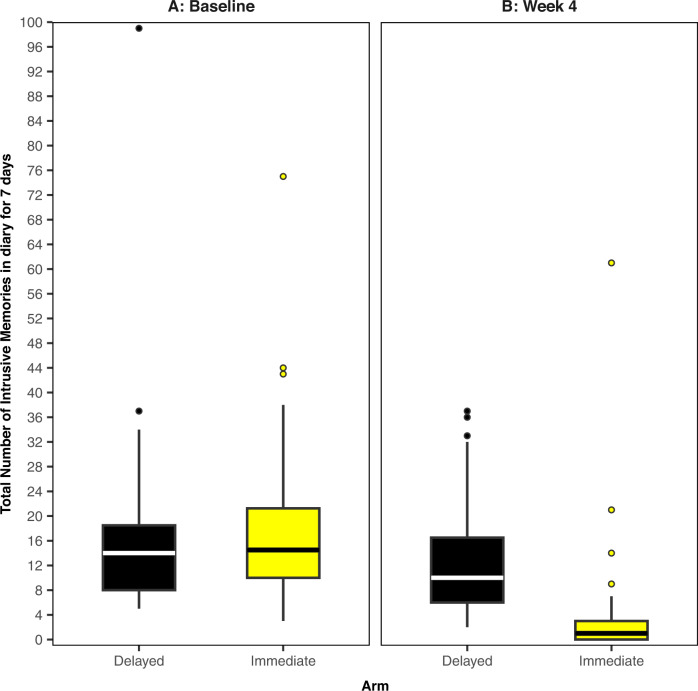
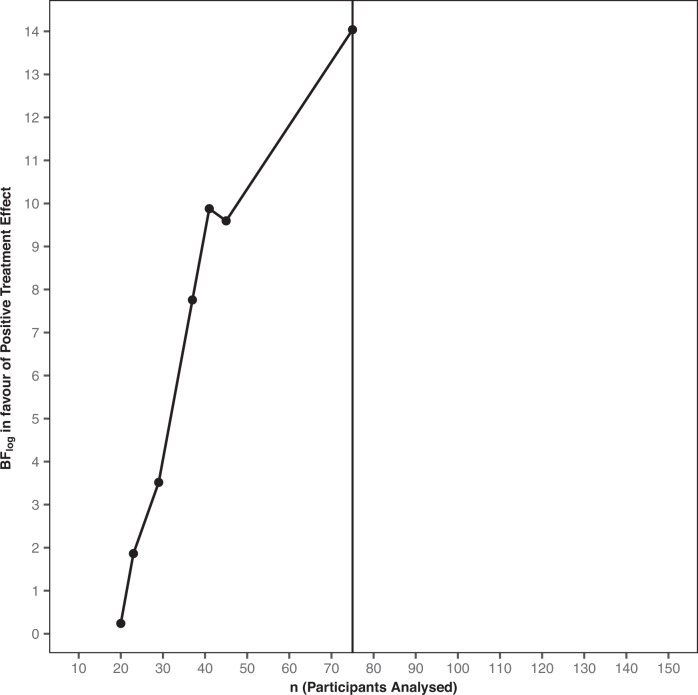
Intensive care unit (ICU) staff continue to face recurrent work-related traumatic events throughout the COVID-19 pandemic. Intrusive memories (IMs) of such traumatic events comprise sensory image-based memories. Harnessing research on preventing IMs with a novel behavioural intervention on the day of trauma, here we take critical next steps in developing this approach as a treatment for ICU staff who are already experiencing IMs days, weeks, or months post-trauma. To address the urgent need to develop novel mental health interventions, we used Bayesian statistical approaches to optimise a brief imagery-competing task intervention to reduce the number of IMs. We evaluated a digitised version of the intervention for remote, scalable delivery. We conducted a two-arm, parallel-group, randomised, adaptive Bayesian optimisation trial. Eligible participants worked clinically in a UK NHS ICU during the pandemic, experienced at least one work-related traumatic event, and at least three IMs in the week prior to recruitment. Participants were randomised to receive immediate or delayed (after 4 weeks) access to the intervention. Primary outcome was the number of IMs of trauma during week 4, controlling for baseline week. Analyses were conducted on an intention-to-treat basis as a between-group comparison. Prior to final analysis, sequential Bayesian analyses were conducted (n = 20, 23, 29, 37, 41, 45) to inform early stopping of the trial prior to the planned maximum recruitment (n = 150). Final analysis (n = 75) showed strong evidence for a positive treatment effect (Bayes factor, BF = 1.25 × 106): the immediate arm reported fewer IMs (median = 1, IQR = 0-3) than the delayed arm (median = 10, IQR = 6-16.5). With further digital enhancements, the intervention (n = 28) also showed a positive treatment effect (BF = 7.31). Sequential Bayesian analyses provided evidence for reducing IMs of work-related trauma for healthcare workers. This methodology also allowed us to rule out negative effects early, reduced the planned maximum sample size, and allowed evaluation of enhancements. Trial Registration NCT04992390 ( www.clinicaltrials.gov ).
© 2023. The Author(s).
Conflict of interest statement
The study was funded by the Wellcome Trust (223016/Z/21/Z). JK is shareholder and director of P1vital Products Ltd which is the study sponsor and manufacturer of i-spero®. VR and LI are employed by P1vital Products Ltd. MBB is an adjunct member of the DMC. CS salary is partly funded by National Institute for Health Research (NIHR133788) and Medical Research Council (MR/S035753/1 and MR/X005070/1). TJ is supported by a grant from UK Medical Research Council (MC_UU_00002/14). EAH salary is part funded by Wellcome Trust (223016/Z/21/Z) via consultancy to P1vital Products Ltd. EAH is on the Board of Trustees of the MQ Foundation. EAH also receives funding from the Swedish Research Council, Rannís The Icelandic Research Fund, OAK foundation, The Lupina Foundation and AFA Försäkring. EAH developed the intervention approach and training in using it (Anenome™). EAH receives book royalties from Guildford Press and Oxford University Press, and receives occasional honoraria for conference keynotes and clinical workshops. All other authors declare no competing interests.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed., vol. 21. Washington DC: American Psychiatric Publishing, 2013.
-
- Colville G, Hammond J, Perkins-Porras L. Post-traumatic stress symptoms in intensive care staff working in adult and paediatric settings. Crit Care. 2015;19:P531.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
