

The utility of the Rapid Emergency Medicine Score (REMS) compared with three other early warning scores in predicting in-hospital mortality among COVID-19 patients in the emergency department: a multicenter validation study
- PMID: 37101141
- PMCID: PMC10132401
- DOI: 10.1186/s12873-023-00814-w
The utility of the Rapid Emergency Medicine Score (REMS) compared with three other early warning scores in predicting in-hospital mortality among COVID-19 patients in the emergency department: a multicenter validation study
Abstract
Background: Many early warning scores (EWSs) have been validated to prognosticate adverse outcomes of COVID-19 in the Emergency Department (ED), including the quick Sequential Organ Failure Assessment (qSOFA), the Modified Early Warning Score (MEWS), and the National Early Warning Score (NEWS). However, the Rapid Emergency Medicine Score (REMS) has not been widely validated for this purpose. We aimed to assess and compare the prognostic utility of REMS with that of qSOFA, MEWS, and NEWS for predicting mortality in emergency COVID-19 patients.
Methods: We conducted a multi-center retrospective study at five EDs of various levels of care in Thailand. Adult patients visiting the ED who tested positive for COVID-19 prior to ED arrival or within the index hospital visit between January and December 2021 were included. Their EWSs at ED arrival were calculated and analysed. The primary outcome was all-cause in-hospital mortality. The secondary outcome was mechanical ventilation.
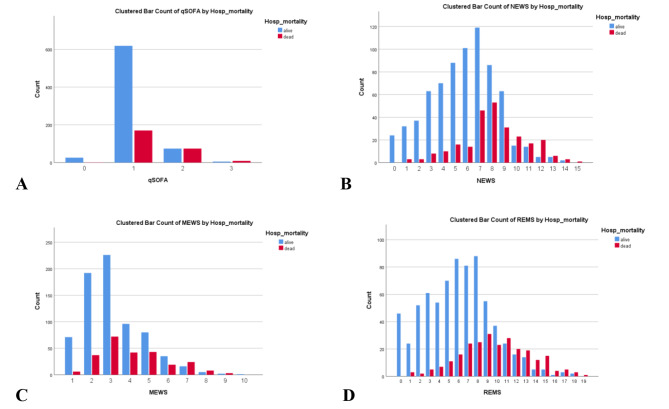
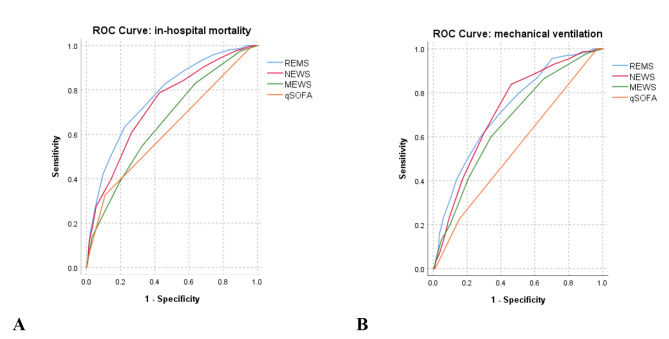
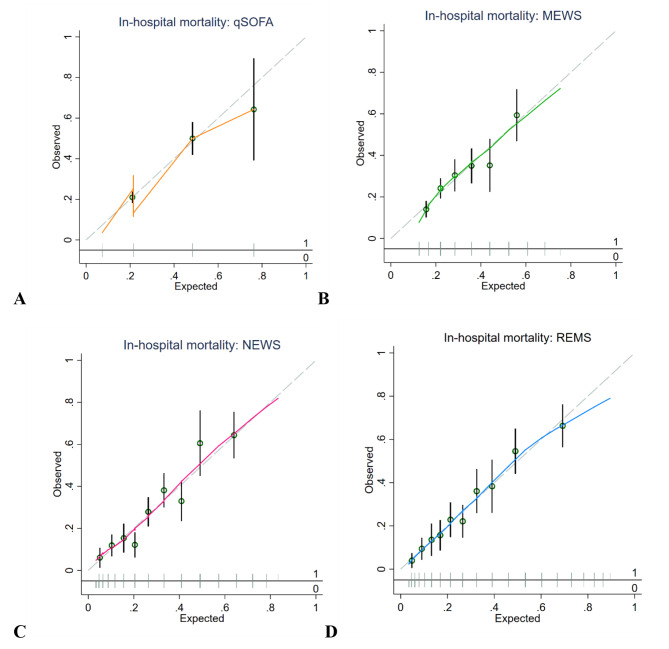
Results: A total of 978 patients were included in the study; 254 (26%) died at hospital discharge, and 155 (15.8%) were intubated. REMS yielded the highest discrimination capacity for in-hospital mortality (the area under the receiver operator characteristics curves (AUROC) 0.771 (95% confidence interval (CI) 0.738, 0.804)), which was significantly higher than qSOFA (AUROC 0.620 (95%CI 0.589, 0.651); p < 0.001), MEWS (AUROC 0.657 (95%CI 0.619, 0.694); p < 0.001), and NEWS (AUROC 0.732 (95%CI 0.697, 0.767); p = 0.037). REMS was also the best EWS in terms of calibration, overall model performance, and balanced diagnostic accuracy indices at its optimal cutoff. REMS also performed better than other EWSs for mechanical ventilation.
Conclusion: REMS was the early warning score with the highest prognostic utility as it outperformed qSOFA, MEWS, and NEWS in predicting in-hospital mortality in COVID-19 patients in the ED.
Keywords: Early warning score; Rapid emergency medicine score; covid-19.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare no conflicts of interest.
Figures
Similar articles
-
The utility of the rapid emergency medicine score (REMS) compared with SIRS, qSOFA and NEWS for Predicting in-hospital Mortality among Patients with suspicion of Sepsis in an emergency department.BMC Emerg Med. 2021 Jan 7;21(1):2. doi: 10.1186/s12873-020-00396-x. BMC Emerg Med. 2021. PMID: 33413139 Free PMC article.
-
Predicting intensive care unit admission and death for COVID-19 patients in the emergency department using early warning scores.Resuscitation. 2020 Nov;156:84-91. doi: 10.1016/j.resuscitation.2020.08.124. Epub 2020 Sep 9. Resuscitation. 2020. PMID: 32918985 Free PMC article.
-
Comparison the accuracy of early warning scores with qSOFA and SIRS for predicting sepsis in the emergency department.Am J Emerg Med. 2021 Aug;46:284-288. doi: 10.1016/j.ajem.2020.07.077. Epub 2020 Aug 7. Am J Emerg Med. 2021. PMID: 33046318
-
Comparison of qSOFA and Hospital Early Warning Scores for prognosis in suspected sepsis in emergency department patients: a systematic review.Emerg Med J. 2022 Apr;39(4):284-294. doi: 10.1136/emermed-2020-210416. Epub 2021 Aug 17. Emerg Med J. 2022. PMID: 34404680
-
Prognostic value of early warning scores in the emergency department (ED) and acute medical unit (AMU): A narrative review.Eur J Intern Med. 2017 Nov;45:20-31. doi: 10.1016/j.ejim.2017.09.027. Epub 2017 Oct 7. Eur J Intern Med. 2017. PMID: 28993097 Review.
Cited by
-
Predicting Mortality for COVID-19 Patients Admitted to an Emergency Department Using Early Warning Scores in Poland.Healthcare (Basel). 2024 Mar 19;12(6):687. doi: 10.3390/healthcare12060687. Healthcare (Basel). 2024. PMID: 38540650 Free PMC article.
-
ANCOC Score to Predict Mortality in Different SARS-CoV-2 Variants and Vaccination Status.J Clin Med. 2023 Sep 8;12(18):5838. doi: 10.3390/jcm12185838. J Clin Med. 2023. PMID: 37762779 Free PMC article.
-
Presepsin as a prognostic biomarker in COVID-19 patients: combining clinical scoring systems and laboratory inflammatory markers for outcome prediction.Virol J. 2024 Apr 26;21(1):96. doi: 10.1186/s12985-024-02367-1. Virol J. 2024. PMID: 38671532 Free PMC article.
-
Reevaluation of prognostic and severity indicators for COVID-19 patients in the emergency department.Ann Med. 2024 Dec;56(1):2417178. doi: 10.1080/07853890.2024.2417178. Epub 2024 Oct 22. Ann Med. 2024. PMID: 39435611 Free PMC article.
-
Evaluation of patients with decreased general condition and comparing HOTEL, WPS, and REMS for mortality prediction.Sci Rep. 2025 Apr 8;15(1):11956. doi: 10.1038/s41598-025-97386-5. Sci Rep. 2025. PMID: 40200107 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
