

Cognitive impairment according to Montreal Cognitive Assessment independently predicts the ability of chronic obstructive pulmonary disease patients to maintain proper inhaler technique
- PMID: 37101175
- PMCID: PMC10131352
- DOI: 10.1186/s12890-023-02448-x
Cognitive impairment according to Montreal Cognitive Assessment independently predicts the ability of chronic obstructive pulmonary disease patients to maintain proper inhaler technique
Abstract
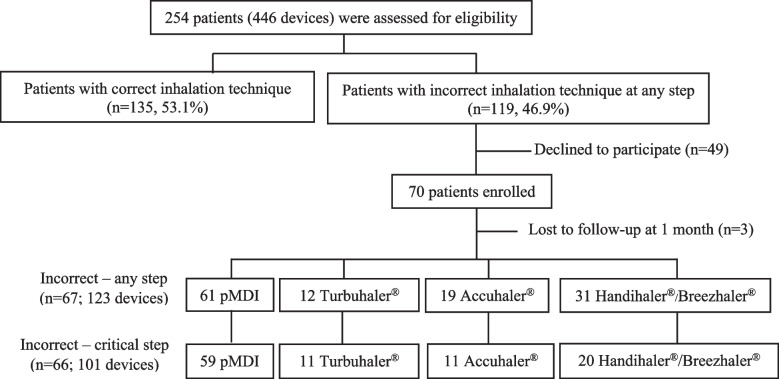
Background: Maintaining correct inhaler technique is crucial in the management of chronic obstructive pulmonary disease (COPD). We aimed to investigate the inhaler technique in patients with COPD, to compare it immediately after and at 1 month after training, and to identify the predictors of incorrect inhaler use at 1 month after training.
Methods: This prospective study was conducted at the COPD clinic of Siriraj Hospital (Bangkok, Thailand). Patients demonstrating improper inhaler use were trained face-to-face by pharmacists. Inhaler technique was re-assessed immediately after and at 1 month after training. The Montreal Cognitive Assessment (MoCA) score, pulmonary function tests, 6-min walk distance (6 MWD), modified Medical Research Council scale score, and COPD Assessment Test (CAT) score were evaluated.
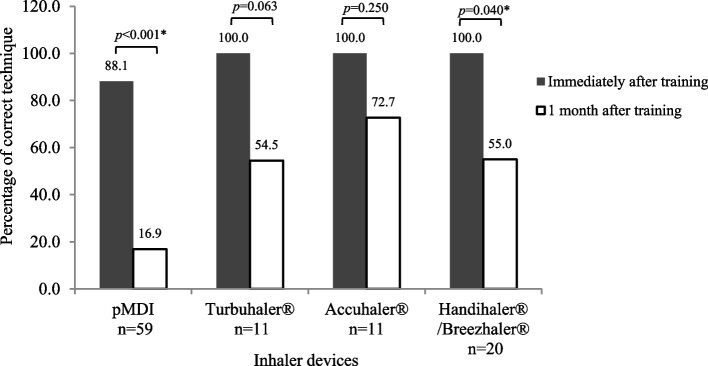
Results: Sixty-six patients with COPD who demonstrated at least one critical error during the use of any controller inhaler were enrolled. The mean age was 73.0 ± 9.0 years, and 75.8% patients had moderate/severe COPD. Immediately after training, all patients used dry powder inhalers correctly and 88.1% used pressurized metered-dose inhalers correctly. At 1 month, the number of patients demonstrating the correct technique decreased across all devices. Multivariable analysis revealed that MoCA score ≤ 16 was independently associated with a critical error at 1 month after training (adjusted odds ratio: 12.7, 95% confidence interval: 1.8-88.2, p = 0.010). At 1 month, CAT score (11.4 ± 8.9 vs. 8.4 ± 5.5, p = 0.018) and 6 MWD (351 ± 93 m vs. 372 ± 92 m, p = 0.009) had significantly improved in patients demonstrating the correct technique, and CAT score met the minimal clinically important difference.
Conclusions: Face-to-face training by pharmacists improved patient performance. However, the number of patients following proper technique had decreased at 1 month after training. Cognitive impairment (MoCA score ≤ 16) independently predicted the ability of COPD patients to maintain proper inhaler technique. Assessment of cognitive function combined with technical re-assessment and repeated training should improve COPD management.
Keywords: Chronic obstructive pulmonary disease; Cognitive impairment; Health status; Incorrect inhaler use; Montreal Cognitive Assessment; Pharmacist.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Pharmacists' training to improve inhaler technique of patients with COPD in Vietnam.Int J Chron Obstruct Pulmon Dis. 2018 Jun 11;13:1863-1872. doi: 10.2147/COPD.S163826. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29928117 Free PMC article.
-
Technical Evaluation of Soft Mist Inhaler Use in Patients with Chronic Obstructive Pulmonary Disease: A Cross-Sectional Study.Int J Chron Obstruct Pulmon Dis. 2020 Jun 22;15:1471-1479. doi: 10.2147/COPD.S253338. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32606655 Free PMC article.
-
Addressing inhaler technique challenges in cognitively impaired chronic obstructive pulmonary disease patients: the impact of customized training programs.Monaldi Arch Chest Dis. 2025 Jan 8. doi: 10.4081/monaldi.2025.3213. Online ahead of print. Monaldi Arch Chest Dis. 2025. PMID: 39783830
-
Inhaler Competence in Nepalese Patients with Asthma and Chronic Obstructive Pulmunory Disease: A Systematic Review.J Nepal Health Res Counc. 2022 Nov 2;20(2):279-288. doi: 10.33314/jnhrc.v20i02.4113. J Nepal Health Res Counc. 2022. PMID: 36550701
-
Inhaled drug delivery in the hands of the patient.J Aerosol Med Pulm Drug Deliv. 2014 Dec;27(6):414-8. doi: 10.1089/jamp.2014.1132. J Aerosol Med Pulm Drug Deliv. 2014. PMID: 25238005 Review.
Cited by
-
Breaking down barriers to COPD management in primary care: applying the updated 2023 Canadian Thoracic Society guideline for pharmacotherapy.Front Med (Lausanne). 2024 Aug 6;11:1416163. doi: 10.3389/fmed.2024.1416163. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39165372 Free PMC article. Review.
-
Construction of a prediction and visualization system for cognitive impairment in elderly COPD patients based on self-assigning feature weights and residual evolution model.Front Artif Intell. 2025 Feb 7;8:1473223. doi: 10.3389/frai.2025.1473223. eCollection 2025. Front Artif Intell. 2025. PMID: 39991464 Free PMC article.
-
The use of the MoCA in cognitive impairment for older patients with Chronic Obstructive Pulmonary disease: A preliminary study.Sci Prog. 2025 Jul-Sep;108(3):368504251347114. doi: 10.1177/00368504251347114. Epub 2025 Jul 21. Sci Prog. 2025. PMID: 40692303 Free PMC article.
-
Recalibrating Perceptions and Attitudes Toward Nebulizers versus Inhalers for Maintenance Therapy in COPD: Past as Prologue.Int J Chron Obstruct Pulmon Dis. 2024 Nov 28;19:2571-2586. doi: 10.2147/COPD.S491275. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39629181 Free PMC article. Review.
-
Comparative effects of square-stepping and strengthening exercises on cognitive and balance functions in chronic obstructive pulmonary disease: a randomized clinical trial.PeerJ. 2025 Jul 30;13:e19792. doi: 10.7717/peerj.19792. eCollection 2025. PeerJ. 2025. PMID: 40755788 Free PMC article. Clinical Trial.
References
-
- Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi: 10.1164/rccm.201204-0596PP. - DOI - PubMed
-
- Crompton GK, Barnes PJ, Broeders M, Corrigan C, Corbetta L, Dekhuijzen R, Dubus JC, Magnan A, Massone F, Sanchis J, et al. The need to improve inhalation technique in Europe: a report from the Aerosol Drug Management Improvement Team. Respir Med. 2006;100(9):1479–1494. doi: 10.1016/j.rmed.2006.01.008. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
