

Early non-invasive ventilation and high-flow nasal oxygen therapy for preventing endotracheal intubation in hypoxemic blunt chest trauma patients: the OptiTHO randomized trial
- PMID: 37101272
- PMCID: PMC10131545
- DOI: 10.1186/s13054-023-04429-2
Early non-invasive ventilation and high-flow nasal oxygen therapy for preventing endotracheal intubation in hypoxemic blunt chest trauma patients: the OptiTHO randomized trial
Abstract
Background: The benefit-risk ratio of prophylactic non-invasive ventilation (NIV) and high-flow nasal oxygen therapy (HFNC-O2) during the early stage of blunt chest trauma remains controversial because of limited data. The main objective of this study was to compare the rate of endotracheal intubation between two NIV strategies in high-risk blunt chest trauma patients.
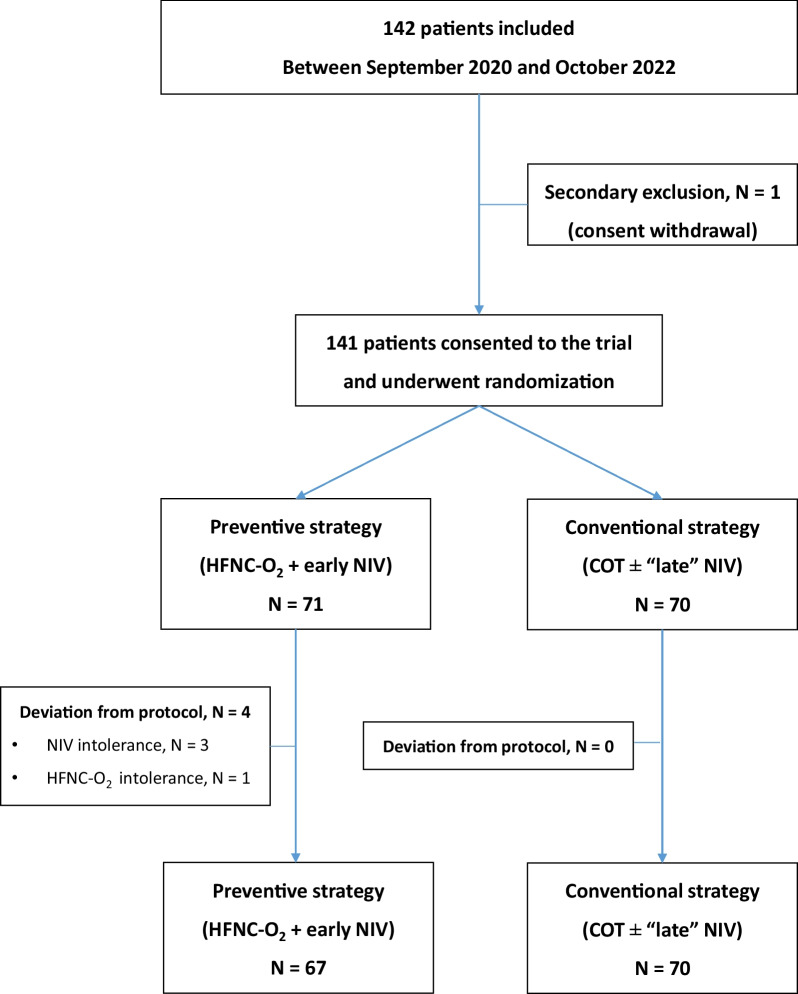
Methods: The OptiTHO trial was a randomized, open-label, multicenter trial over a two-year period. Every adult patients admitted in intensive care unit within 48 h after a high-risk blunt chest trauma (Thoracic Trauma Severity Score ≥ 8), an estimated PaO2/FiO2 ratio < 300 and no evidence of acute respiratory failure were eligible for study enrollment (Clinical Trial Registration: NCT03943914). The primary objective was to compare the rate of endotracheal intubation for delayed respiratory failure between two NIV strategies: i) a prompt association of HFNC-O2 and "early" NIV in every patient for at least 48 h with vs. ii) the standard of care associating COT and "late" NIV, indicated in patients with respiratory deterioration and/or PaO2/FiO2 ratio ≤ 200 mmHg. Secondary outcomes were the occurrence of chest trauma-related complications (pulmonary infection, delayed hemothorax or moderate-to-severe ARDS).
Results: Study enrollment was stopped for futility after a 2-year study period and randomization of 141 patients. Overall, 11 patients (7.8%) required endotracheal intubation for delayed respiratory failure. The rate of endotracheal intubation was not significantly lower in patients treated with the experimental strategy (7% [5/71]) when compared to the control group (8.6% [6/70]), with an adjusted OR = 0.72 (95%IC: 0.20-2.43), p = 0.60. The occurrence of pulmonary infection, delayed hemothorax or delayed ARDS was not significantly lower in patients treated by the experimental strategy (adjusted OR = 1.99 [95%IC: 0.73-5.89], p = 0.18, 0.85 [95%IC: 0.33-2.20], p = 0.74 and 2.14 [95%IC: 0.36-20.77], p = 0.41, respectively).
Conclusion: A prompt association of HFNC-O2 with preventive NIV did not reduce the rate of endotracheal intubation or secondary respiratory complications when compared to COT and late NIV in high-risk blunt chest trauma patients with non-severe hypoxemia and no sign of acute respiratory failure.
Clinical trial registration: NCT03943914, Registered 7 May 2019.
Keywords: Chest trauma; High-flow nasal oxygen therapy; Intensive care; Non-invasive ventilation; Respiratory failure.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
