

Case Reports
doi: 10.1016/j.hrcr.2023.01.005.
eCollection 2023 Apr.
Atrial-His-atrial and atrial-His-His-atrial responses during slow-fast atrioventricular nodal reentrant tachycardia
Affiliations
- PMID: 37101667
- PMCID: PMC10123928
- DOI: 10.1016/j.hrcr.2023.01.005
Item in Clipboard
Case Reports
Atrial-His-atrial and atrial-His-His-atrial responses during slow-fast atrioventricular nodal reentrant tachycardia
HeartRhythm Case Rep.
.
No abstract available
Keywords: Atrial overdrive pacing; Atrial-His-His-atrial response; Atrial-His-atrial response; Atrioventricular nodal reentrant tachycardia; Double ventricular response; Junctional tachycardia.
Figures

Different responses to atrial overdrive pacing (AOP) were observed during the tachycardia. A: AOP from the HRA (TCL 489 ms, PCL 475 ms) exhibited an atrial-His-His-atrial response, which was presumably caused by the simultaneous atrioventricular nodal conduction: one conducting via the fast pathway (red solid arrows) and the other via the slow pathway (red dotted arrows). PPI–TCL was 138 ms, which suggested that the HRA was far from the tachycardia circuit. The His electrograms immediately after the stimulus (H1) were directly activated by pacing, whereas the subsequent His electrograms (H2) were activated after penetrating the slow conduction zone. The H1H2 interval was shorter than the TCL. B: AOP from the proximal CS (TCL 489 ms, PCL 475 ms) exhibited an atrial-His-atrial response. PPI–TCL was 66 ms, which suggested that the proximal CS was near the tachycardia circuit. The last captured His (H1) electrograms were the second beat after the stimulus, suggesting the His bundle electrograms were orthodromically captured. The H1H2 interval was similar to the TCL. CS = coronary sinus; HB = His bundle; HRA = high right atrium; PCL = pacing cycle length; PPI = postpacing interval; RVA= right ventricular apex; TCL = tachycardia cycle length.

The possible mechanism of atrial-His-His-atrial (AHHA) and atrial-His-atrial (AHA) responses after an atrial overdrive pacing (AOP) in junctional tachycardia (JT) and atrioventricular nodal reentrant tachycardia (AVNRT). H1 and H2 are defined as the last captured His electrograms with a pacing cycle length (PCL) and the subsequent His electrograms, respectively. A: AOP during JT will transiently suppress the arrhythmia after pacing cessation and the tachycardia will resume with a junctional beat, beginning with a His signal. This will result in an AHHA response, and the H1H2 interval would be longer than the tachycardia cycle length (TCL) owing to the overdrive suppression in automatic cells. B: Contrarily, during AOP of the slow-fast AVNRT, the tachycardia will be entrained, and the anterograde atrioventricular nodal conduction propagates only through the slow pathway (SP) because the fast pathway (FP) is refractory from the retrograde conduction. After pacing cessation, the tachycardia will resume after the last paced beat. The last atrial paced beat during typical AVNRT should conduct anterograde down the SP and exit into the His-Purkinje system while echoing up the FP and exiting into the atrium (A). This would result in an AHA response. In this scenario, the tachycardia would continue during AOP, and the H1H2 interval would be similar to the TCL. C: However, if AOD terminates the tachycardia and the last atrial pacing simultaneously propagates over the fast and slow pathways (ie, double ventricular response), the last atrial paced beat can result in 2 His signals. When an antegrade conduction via SP could retrogradely activate the FP and reinitiate the tachycardia, an AHHA response is observed even in slow-fast AVNRT. The H1H2 interval would be shorter than the TCL, because it corresponds to the difference between antegrade FP and SP conductions. However, if the PCL is much shorter than the TCL, the decremental property of the SP can make the H1H2 interval equal to or longer than the TCL.
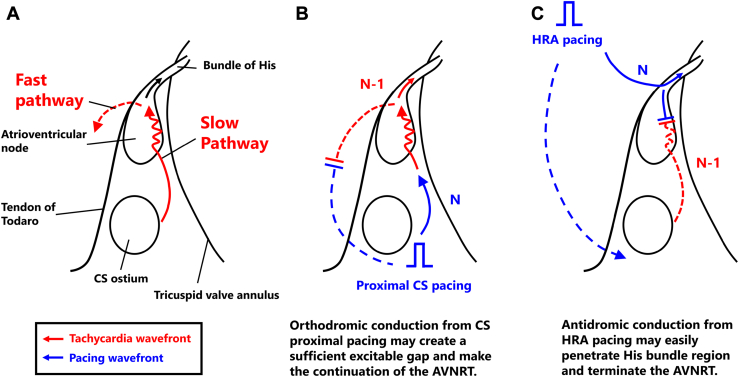
Schematic representations of the activation wavefront during (A) slow-fast atrioventricular nodal reentrant tachycardia (AVNRT) and during atrial overdrive pacing (AOP) from (B) the proximal coronary sinus (CS) and (C) high right atrium (HRA). A: In typical AVNRT, the proximal CS is presumably located on the entrance side of the slow conduction zone (ie, slow pathway). B: The AOP from the entrance side of the slow conduction zone may allow the continuous resetting of the AVNRT by creating an excitable gap in the downstream myocardium. The antidromic wavefront of the first stimulus collides with the tachycardia, whereas its orthodromic counterpart advances the circuit. With the continuation of pacing, the orthodromic wavefront (N–1) after penetrating the slow conduction zone continuously collides with the antidromic wavefront of the subsequent pacing (N). C: Conversely, the HRA is presumably located on the exit side of the slow conduction zone. The antidromic wavefront (antegrade conduction via a fast pathway) would easily collide with the tachycardia wavefront and terminate the AVNRT. Then, the pacing wavefront would easily penetrate the His bundle electrograms via antegrade fast pathway conduction. These phenomena may make the continuation of the tachycardia difficult during AOP.
References
-
- Fan R., Tardos J.G., Almasry I., Barbera S., Rashba E.J., Iwai S. Novel use of atrial overdrive pacing to rapidly differentiate junctional tachycardia from atrioventricular nodal reentrant tachycardia. Heart Rhythm. 2011;8:840–844. - PubMed
-
- Kim S.S., Lal R., Ruffy R. Paroxysmal nonreentrant supraventricular tachycardia due to simultaneous fast and slow pathway conduction in dual atrioventricular node pathways. J Am Coll Cardiol. 1987;10:456–461. - PubMed
-
- Satoh M., Miyajima S., Koyama S., Ishiguro J., Okabe M. Orthodromic capture of the atrial electrogram during transient entrainment of atrioventricular nodal reentrant tachycardia. Circulation. 1993;88:2329–2336. - PubMed
-
- Okumura K., Olshansky B., Henthorn R.W., Epstein A.E., Plumb V.J., Waldo A.L. Demonstration of the presence of slow conduction during sustained ventricular tachycardia in man: use of transient entrainment of the tachycardia. Circulation. 1987;75:369–378. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
