

Neuromotor Treatment of Arthrogenic Muscle Inhibition After Knee Injury or Surgery
- PMID: 37102673
- PMCID: PMC11025506
- DOI: 10.1177/19417381231169285
Neuromotor Treatment of Arthrogenic Muscle Inhibition After Knee Injury or Surgery
Abstract
Background: Persistent weakness of the quadriceps muscles and extension deficit after knee injuries are due to specific alterations in neural excitability - a process known as arthrogenic muscle inhibition (AMI). The effects of a novel neuromotor reprogramming (NR) treatment based on the use of proprioceptive sensations associated with motor imagery and low frequency sounds have not been studied in AMI after knee injuries.
Hypothesis: This study aimed to assess quadriceps electromyographic (EMG) activity and the effects on extension deficits in persons with AMI who completed 1 session of NR treatment. We hypothesized that the NR session would activate the quadriceps and improve extension deficits.
Study design: Case series.
Level of evidence: Level 4.
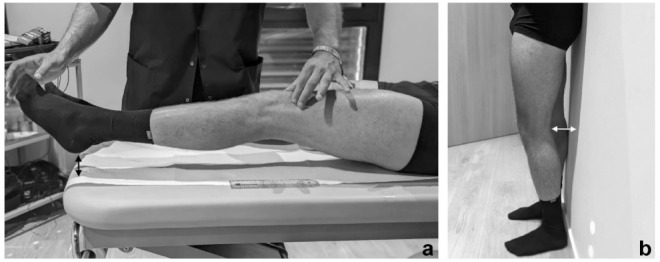
Methods: Between May 1, 2021 and February 28, 2022, patients who underwent knee ligament surgery or sustained a knee sprain with a deficit of >30% of the vastus medialis oblique (VMO) on EMG testing in comparison with the contralateral limb after their initial rehabilitation were included in the study. The maximal voluntary isometric contraction of the VMO measured on EMG, the knee extension deficit (distance between the heel and the table during contraction), and the simple knee value (SKV) were assessed before and immediately after completion of 1 session of NR treatment.
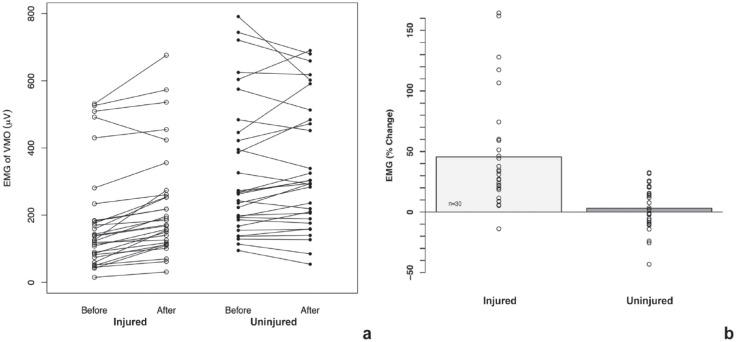
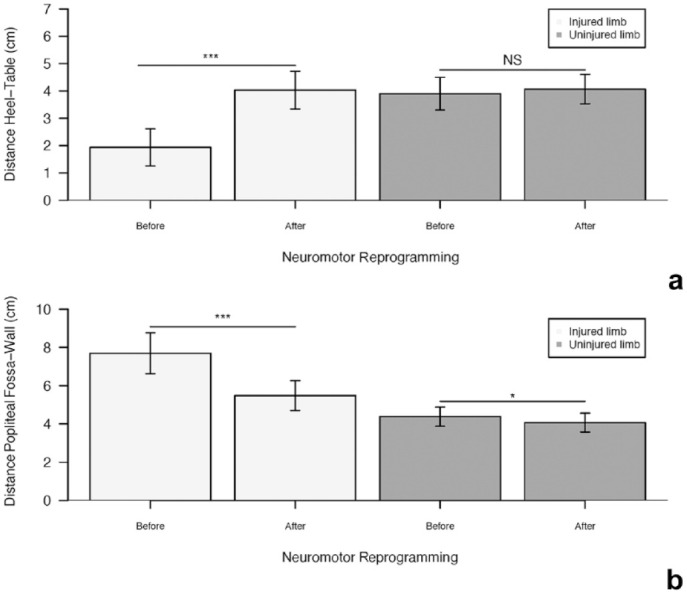
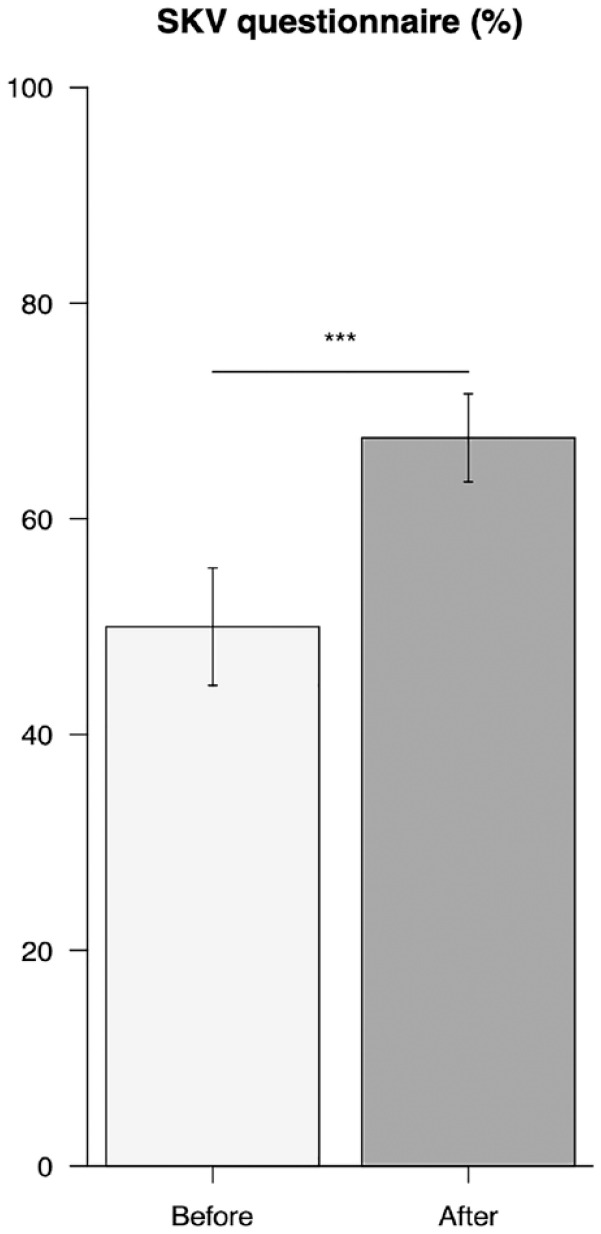
Results: A total of 30 patients with a mean age of 34.6 ± 10.1 years (range, 14-50 years) were included in the study. After the NR session, VMO activation increased significantly, with a mean increase of 45% (P < 0.01). Similarly, the knee extension deficit significantly improved from 4.03 ± 0.69 cm before the treatment to 1.93 ± 0.68 after the treatment (P < 0.01). The SKV was 50 ± 5.43% before the treatment, and this increased to 67.5 ± 4.09% after the treatment (P < 0.01).
Conclusion: Our study indicates that this innovative NR method can improve VMO activation and extension deficits in patients with AMI. Therefore, this method could be considered a safe and reliable treatment modality in patients with AMI after knee injury or surgery.
Clinical relevance: This multidisciplinary treatment modality for AMI can enhance outcomes through the restoration of quadriceps neuromuscular function and subsequent reduction of extension deficits after knee trauma.
Keywords: arthrogenic muscle inhibition; knee; neuromotor reprogramming.
Conflict of interest statement
The following authors declared potential conflicts of interest: T.D.V. received collaborative research funding from Allyane. B.S-C. is a paid consultant for Arthrex and has received royalties from Arthrex.
Figures

References
-
- Andrushko JW, Gould LA, Farthing JP. Contralateral effects of unilateral training: sparing of muscle strength and size after immobilization. Appl Physiol Nutr Metab. 2018;43(11):1131-1139. - PubMed
-
- Bierke S, Abdelativ Y, Hees T, et al.. Risk of arthrofibrosis in anatomical anterior cruciate ligament reconstruction: the role of timing and meniscus suture. Arch Orthop Trauma Surg. 2021;141(5):743-750 - PubMed
-
- Bremner CB, Holcomb WR, Brown CD, Perreault ME. The effectiveness of neuromuscular electrical stimulation in improving voluntary activation of the quadriceps: a critically appraised topic. J Sport Rehab. 2017;26(4):316-323. - PubMed
-
- Clayton RAE, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008;39(12):1338-1344. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
