

A Phase Ib/II Study of Ivosidenib with Venetoclax ± Azacitidine in IDH1-Mutated Myeloid Malignancies
- PMID: 37102976
- PMCID: PMC10320628
- DOI: 10.1158/2643-3230.BCD-22-0205
A Phase Ib/II Study of Ivosidenib with Venetoclax ± Azacitidine in IDH1-Mutated Myeloid Malignancies
Abstract
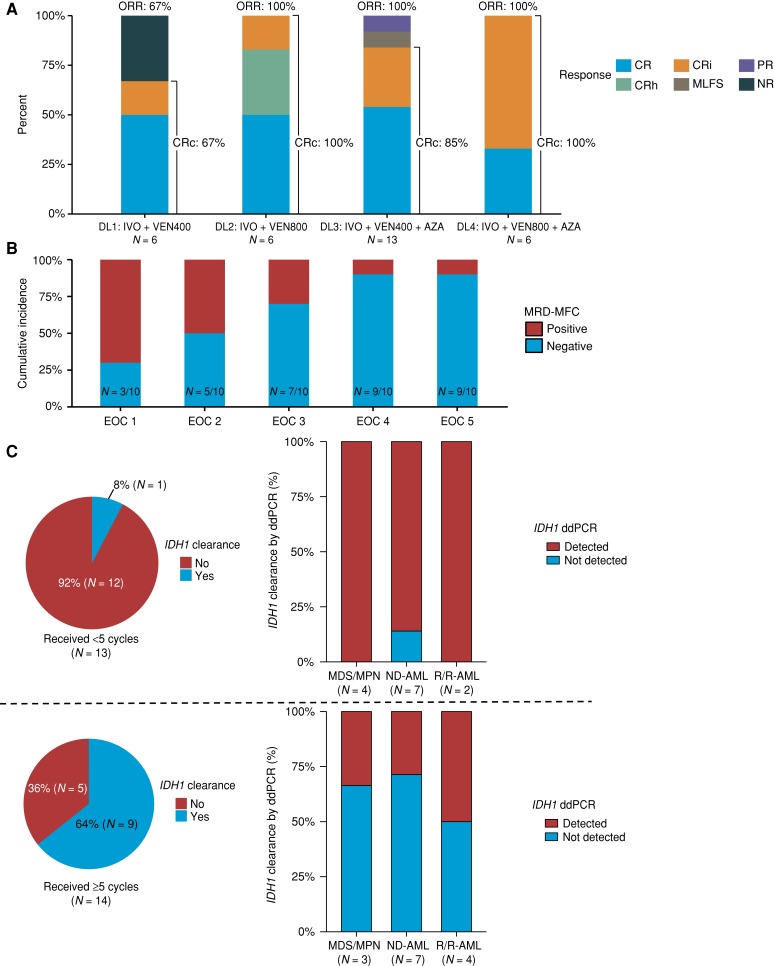
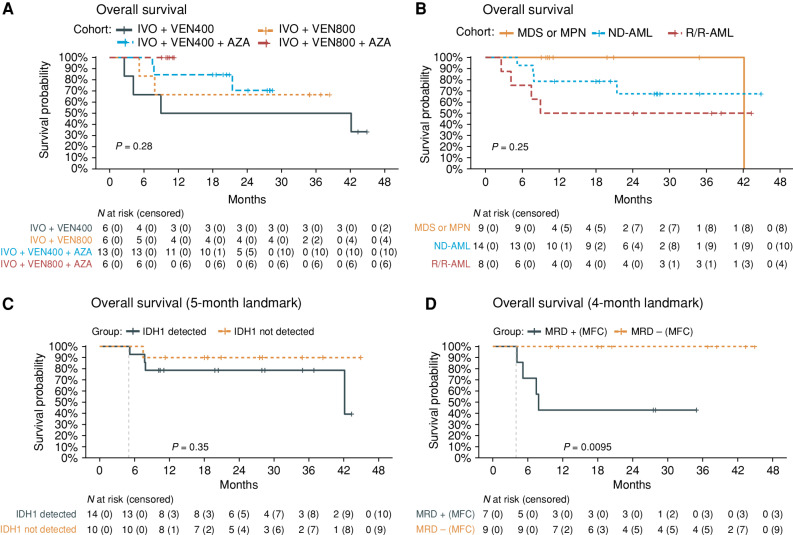
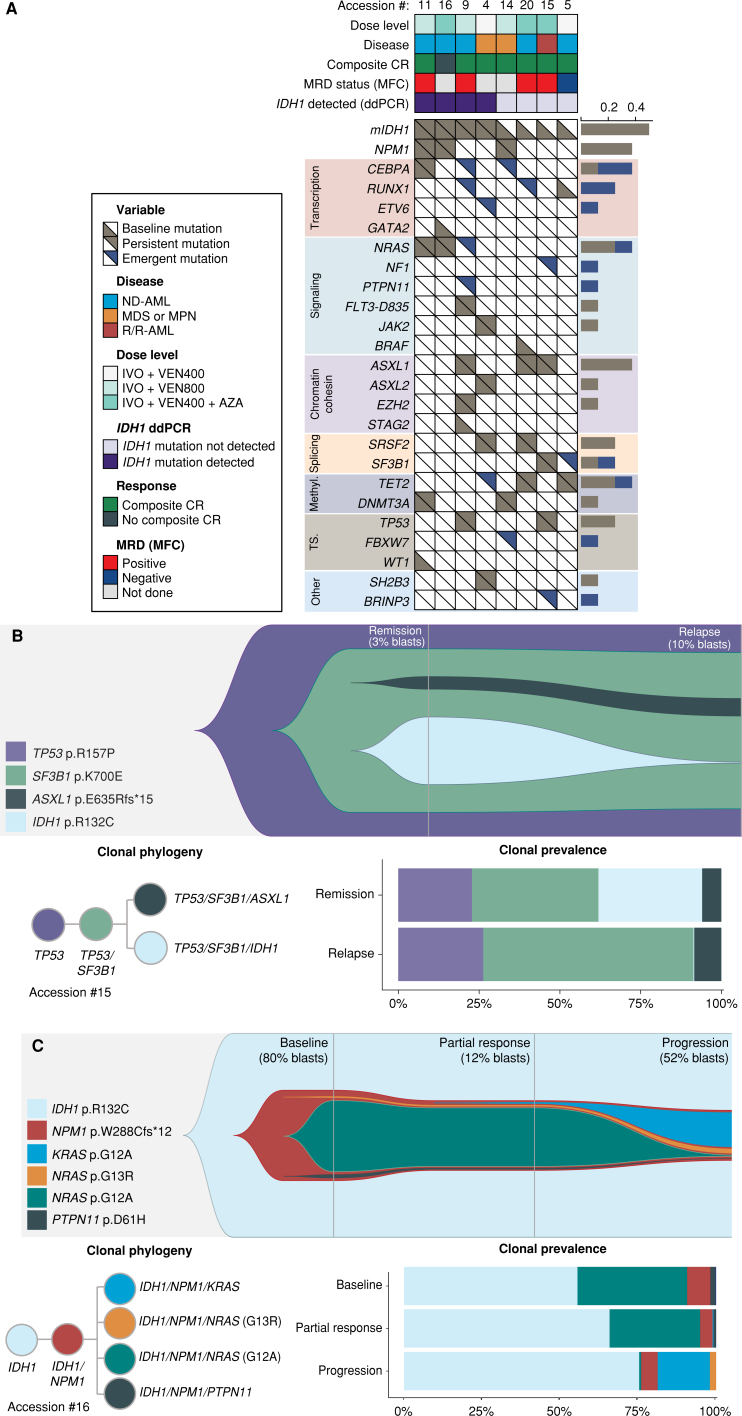
The safety and efficacy of combining the isocitrate dehydrogenase-1 (IDH1) inhibitor ivosidenib (IVO) with the BCL2 inhibitor venetoclax (VEN; IVO + VEN) ± azacitidine (AZA; IVO + VEN + AZA) were evaluated in four cohorts of patients with IDH1-mutated myeloid malignancies (n = 31). Most (91%) adverse events were grade 1 or 2. The maximal tolerated dose was not reached. Composite complete remission with IVO + VEN + AZA versus IVO + VEN was 90% versus 83%. Among measurable residual disease (MRD)-evaluable patients (N = 16), 63% attained MRD--negative remissions; IDH1 mutation clearance occurred in 64% of patients receiving ≥5 treatment cycles (N = 14). Median event-free survival and overall survival were 36 [94% CI, 23-not reached (NR)] and 42 (95% CI, 42-NR) months. Patients with signaling gene mutations appeared to particularly benefit from the triplet regimen. Longitudinal single-cell proteogenomic analyses linked cooccurring mutations, antiapoptotic protein expression, and cell maturation to therapeutic sensitivity of IDH1-mutated clones. No IDH isoform switching or second-site IDH1 mutations were observed, indicating combination therapy may overcome established resistance pathways to single-agent IVO.
Significance: IVO + VEN + AZA is safe and active in patients with IDH1-mutated myeloid malignancies. Combination therapy appears to overcome resistance mechanisms observed with single-agent IDH-inhibitor use, with high MRD-negative remission rates. Single-cell DNA ± protein and time-of-flight mass-cytometry analysis revealed complex resistance mechanisms at relapse, highlighting key pathways for future therapeutic intervention. This article is highlighted in the In This Issue feature, p. 247.
©2023 American Association for Cancer Research.
Figures
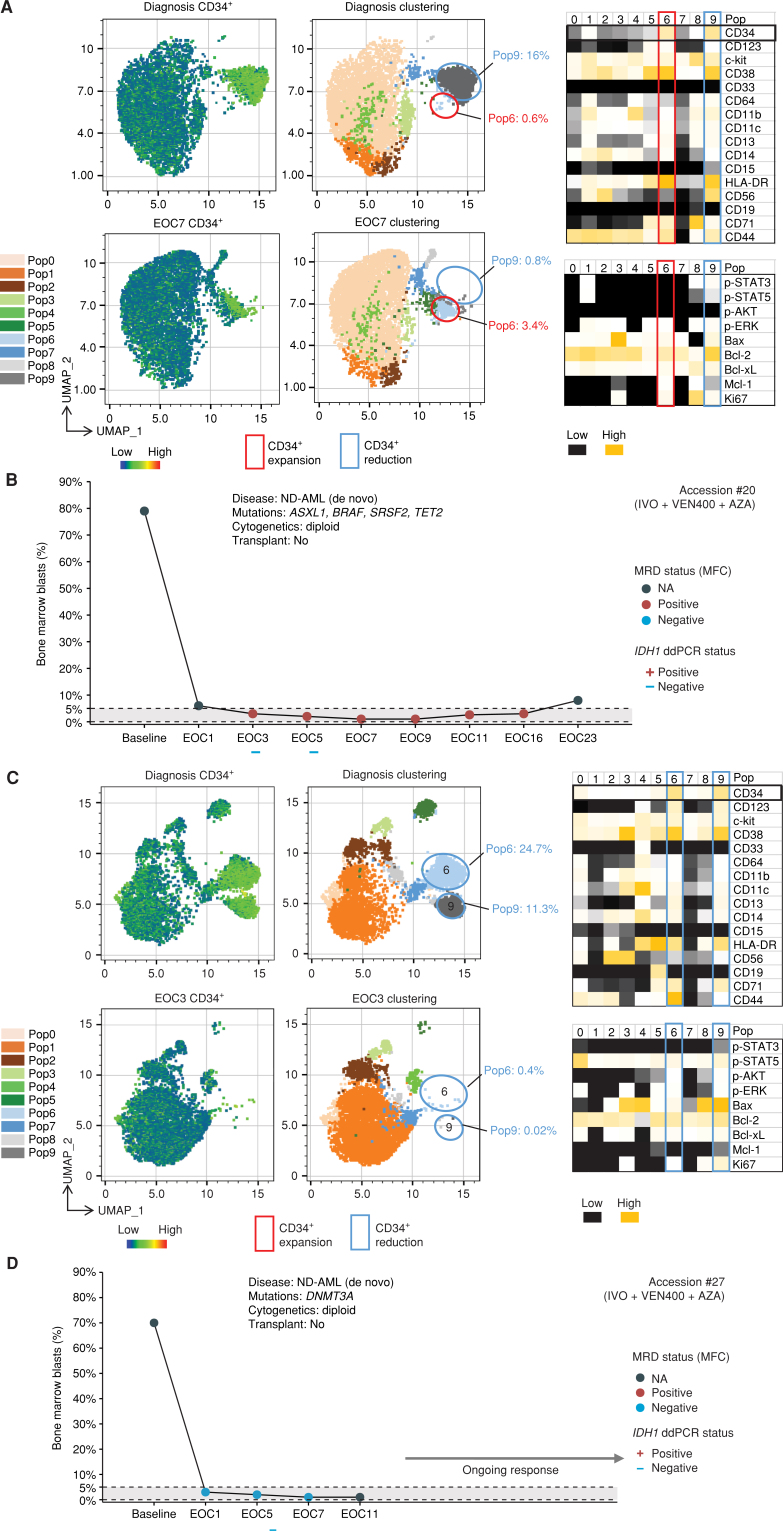
![Figure 4. scDNA + surface protein (DAb-seq) analysis of a patient with ND-AML (accession #20) treated with IVO + VEN + AZA with subsequent deescalation to IVO maintenance therapy revealed dynamic clonal changes secondary to selective pressure of targeted therapy. A–C, Single-cell analysis at diagnosis, in remission [sampled at end of cycle (EOC) 1, 3, 7, and 9] and after relapse (sampled at EOC 26) identified elimination of IDH1-mutated clones following IVO + VEN + AZA treatment, with persistent mutations in background preleukemic genes. D–F, Analysis of the surface proteome revealed a phenotypic shift occurring between diagnosis and relapse (EOC26), with a more primitive immunophenotype identified at relapse following IVO maintenance. G, Paired genotype–phenotype analysis demonstrated the expanding primitive myeloid progenitor clone contributing to relapse did not contain mutated IDH1. H, Bulk next-generation myeloid panel sequencing in this patient identified outgrowth of a RUNX1 mutation at relapse, poorly covered in the scDNA-seq analysis. NK, natural killer.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/b77c/10320628/4a8ac04bcf31/276fig4.jpg)
Comment in
- 2643-3230. doi: 10.1158/2643-3230.BCD-4-4-ITI
References
-
- Paschka P, Schlenk RF, Gaidzik VI, Habdank M, Krönke J, Bullinger L, et al. IDH1 and IDH2 mutations are frequent genetic alterations in acute myeloid leukemia and confer adverse prognosis in cytogenetically normal acute myeloid leukemia with NPM1 mutation without FLT3 internal tandem duplication. J Clin Oncol 2010;28:3636–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MR/R002258/1/MRC_/Medical Research Council/United Kingdom
- L30 CA162036/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- KL2 TR002370/TR/NCATS NIH HHS/United States
- MR/L008963/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00029/8/MRC_/Medical Research Council/United Kingdom
- MC_UU_12009/11/MRC_/Medical Research Council/United Kingdom
- MC_U137961146/MRC_/Medical Research Council/United Kingdom
- R01 CA262636/CA/NCI NIH HHS/United States
- T32 CA009666/CA/NCI NIH HHS/United States
- G1000729/MRC_/Medical Research Council/United Kingdom
- P50 CA100632/CA/NCI NIH HHS/United States
- MC_UU_00016/11/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Miscellaneous
