

Left Ventricle Segmental Longitudinal Strain and Regional Myocardial Work Index Could Help Determine Mitral Valve Prolapse Patients with Increased Risk of Ventricular Arrhythmias
- PMID: 37103060
- PMCID: PMC10145267
- DOI: 10.3390/jcdd10040181
Left Ventricle Segmental Longitudinal Strain and Regional Myocardial Work Index Could Help Determine Mitral Valve Prolapse Patients with Increased Risk of Ventricular Arrhythmias
Abstract
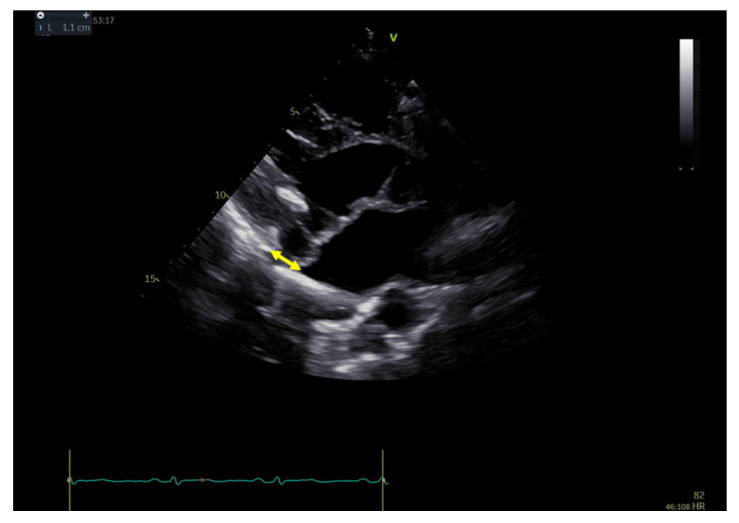
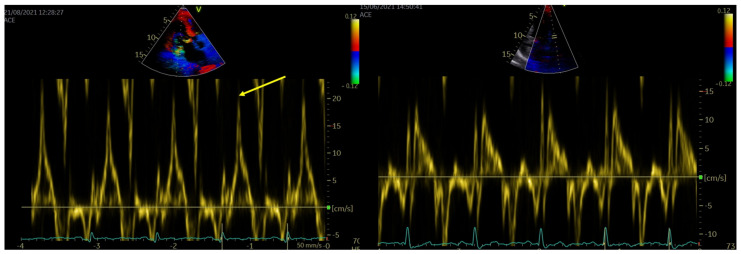
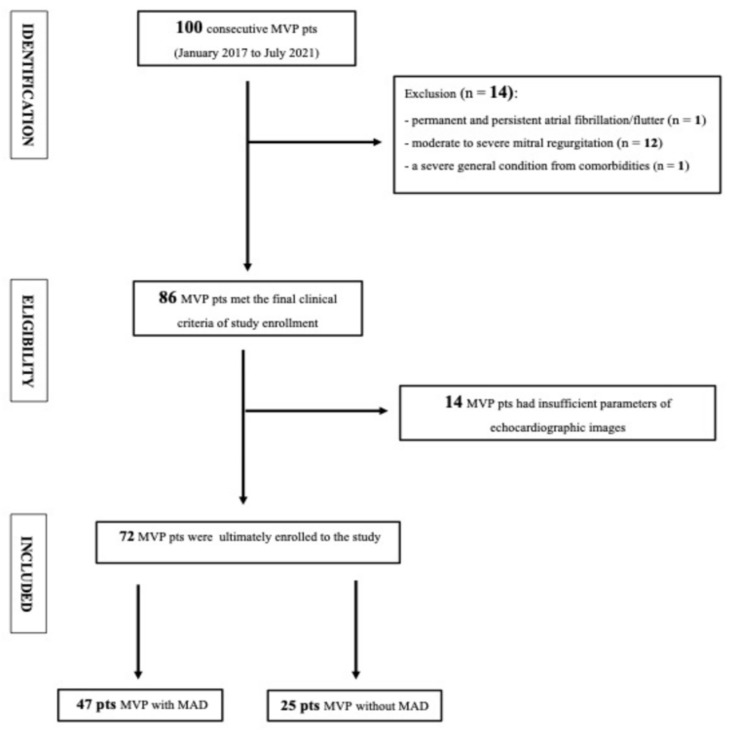
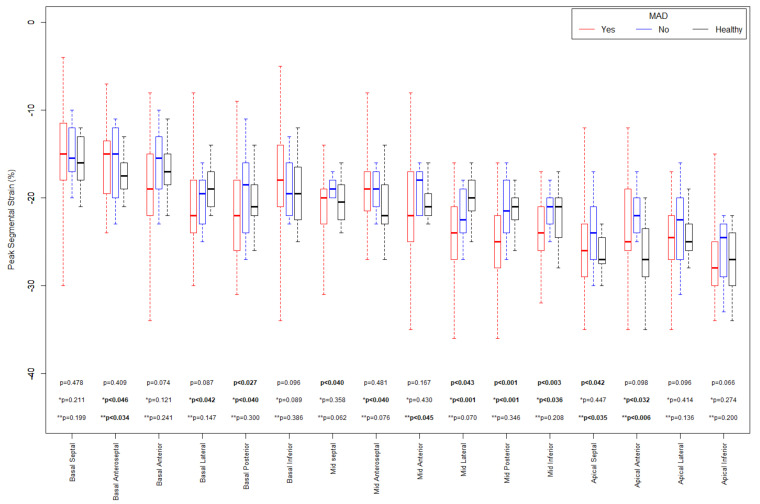
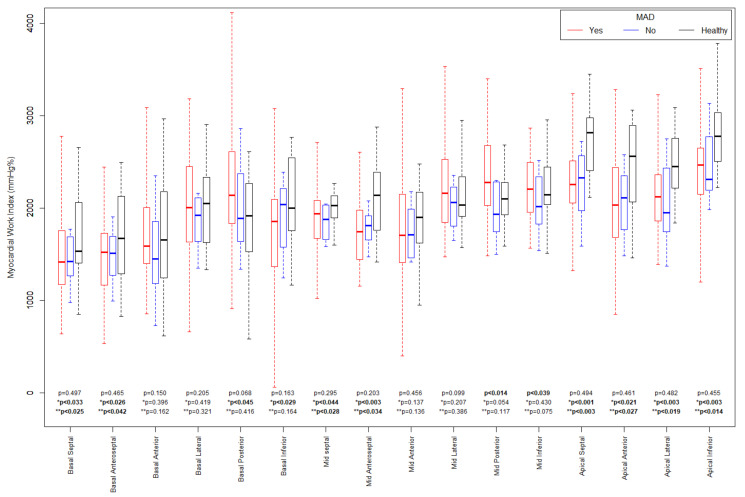
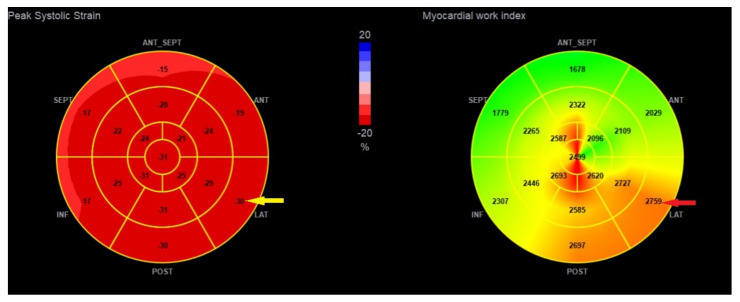
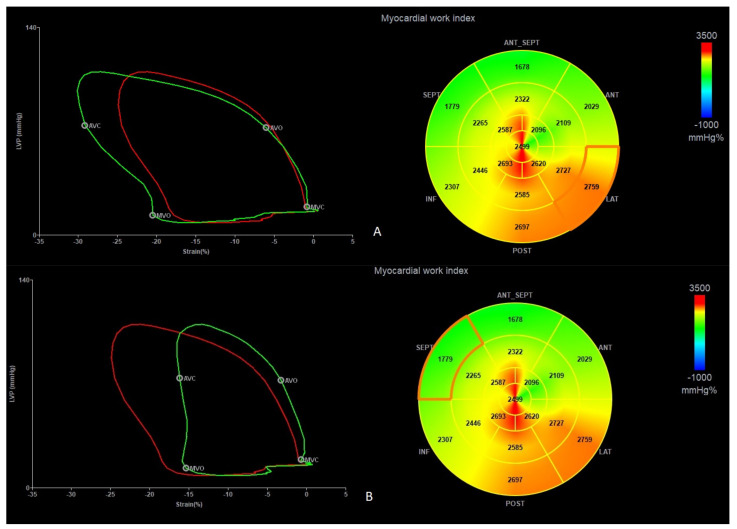
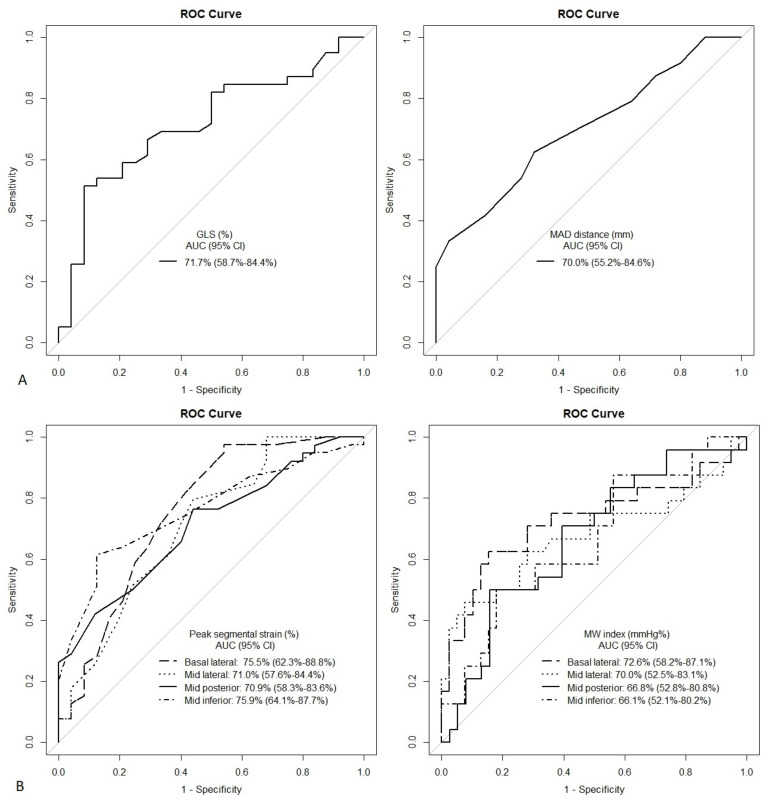
Mitral valve prolapse (MVP) could associate with malignant ventricular arrhythmias (VAs). Mitral annular disjunction, a putative mechanism for an arrhythmic substrate, leads to excessive mobility, stretch, and damage of some segments. Speckle tracking echocardiography (STE), with particular attention to the segmental longitudinal strain and myocardial work index (MWI), could be an indicator of the segments we aimed to check. Seventy-two MVP patients and twenty controls underwent echocardiography. Complex VAs documented prospectively after the enrollment was qualified as the primary endpoint, which was noticed in 29 (40%) patients. Pre-specified cut-off values for peak segmental longitudinal strain (PSS) and segmental MWI for basal lateral (-25%, 2200 mmHg%), mid-lateral (-25%, 2500 mmHg%), mid-posterior (-25%, 2400 mmHg%), and mid-inferior (-23%, 2400 mmHg%) segments were accurate predictors of complex VAs. A combination of PSS and MWI increased the probability of the endpoint, reaching the highest predictive value for the basal lateral segment: odds ratio 32.15 (3.78-273.8), p < 0.001 for PSS ≥ -25% and MWI ≥ 2200 mmHg%. STE may be a valuable tool for assessing the arrhythmic risk in MVP patients. Excessively increased segmental longitudinal strain with an augmented regional myocardial work index identifies patients with the highest risk of complex VAs.
Keywords: longitudinal strain; mitral valve prolapse; myocardial work; nonsustained ventricular tachycardia; speckle tracking echocardiography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Interactions between mitral valve and left ventricle analysed by 2D speckle tracking in patients with mitral valve prolapse: one more piece to the puzzle.Eur Heart J Cardiovasc Imaging. 2017 Mar 1;18(3):323-331. doi: 10.1093/ehjci/jew075. Eur Heart J Cardiovasc Imaging. 2017. PMID: 27099279
-
Abnormal Mechanics Relate to Myocardial Fibrosis and Ventricular Arrhythmias in Patients With Mitral Valve Prolapse.Circ Cardiovasc Imaging. 2023 Apr;16(4):e014963. doi: 10.1161/CIRCIMAGING.122.014963. Epub 2023 Apr 18. Circ Cardiovasc Imaging. 2023. PMID: 37071717 Free PMC article.
-
Basal Left Ventricular Dilatation and Reduced Contraction in Patients With Mitral Valve Prolapse Can Be Secondary to Annular Dilatation: Preoperative and Postoperative Speckle-Tracking Echocardiographic Study on Left Ventricle and Mitral Valve Annulus Interaction.Circ Cardiovasc Imaging. 2016 Oct;9(10):e005113. doi: 10.1161/CIRCIMAGING.115.005113. Circ Cardiovasc Imaging. 2016. PMID: 27729364
-
Mitral Valve Prolapse, Ventricular Arrhythmias, and Sudden Death.Circulation. 2019 Sep 10;140(11):952-964. doi: 10.1161/CIRCULATIONAHA.118.034075. Epub 2019 Sep 9. Circulation. 2019. PMID: 31498700 Review.
-
Transthoracic echocardiography for arrhythmic mitral valve prolapse: Phenotypic characterization as first step.Echocardiography. 2022 Sep;39(9):1158-1170. doi: 10.1111/echo.15439. Epub 2022 Aug 27. Echocardiography. 2022. PMID: 36029124 Review.
Cited by
-
Echocardiographic assessment of left ventricular mechanics in individuals with mitral valve prolapse: a systematic review and meta-analysis.Int J Cardiovasc Imaging. 2024 Aug;40(8):1617-1629. doi: 10.1007/s10554-024-03179-8. Epub 2024 Jul 8. Int J Cardiovasc Imaging. 2024. PMID: 38976111
-
Arrhythmic mitral valve complex: diagnostic and therapeutic approach.Arch Cardiol Mex. 2025;95(2):225-234. doi: 10.24875/ACM.24000097. Arch Cardiol Mex. 2025. PMID: 40445931 Free PMC article. Review. English.
References
-
- Sriram C.S., Syed F.F., Ferguson M.E., Johnson J.N., Enriquez-Sarano M., Cetta F., Cannon B.C., Asirvatham S.J., Ackerman M.J. Malignant bileaflet mitral valve prolapse syndrome in patients with otherwise idiopathic out-of-hospital cardiac arrest. J. Am. Coll. Cardiol. 2013;62:222–230. doi: 10.1016/j.jacc.2013.02.060. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
