

Assessment of the HER2DX Assay in Patients With ERBB2-Positive Breast Cancer Treated With Neoadjuvant Paclitaxel, Trastuzumab, and Pertuzumab
- PMID: 37103927
- PMCID: PMC10141272
- DOI: 10.1001/jamaoncol.2023.0181
Assessment of the HER2DX Assay in Patients With ERBB2-Positive Breast Cancer Treated With Neoadjuvant Paclitaxel, Trastuzumab, and Pertuzumab
Abstract
Importance: Patients with early-stage ERBB2 (formerly HER2)-positive breast cancer (ERBB2+ BC) who experience a pathologic complete response (pCR) after receiving neoadjuvant therapy have favorable survival outcomes. Predicting the likelihood of pCR may help optimize neoadjuvant therapy.
Objective: To test the ability of the HER2DX assay to predict the likelihood of pCR in patients with early-stage ERBB2+ BC who are receiving deescalated neoadjuvant therapy.
Design, setting, and participants: In this diagnostic/prognostic study, the HER2DX assay was administered on pretreatment tumor biopsy samples from patients enrolled in the single-arm, multicenter, prospective phase 2 DAPHNe clinical trial who had newly diagnosed stage II to III ERBB2+ BC that was treated with neoadjuvant paclitaxel weekly for 12 weeks plus trastuzumab and pertuzumab every 3 weeks for 4 cycles.
Interventions and exposures: The HER2DX assay is a classifier derived from gene expression and limited clinical features that provides 2 independent scores to predict prognosis and likelihood of pCR in patients with early-stage ERBB2+ BC. The assay was administered on baseline tumor samples from 80 of 97 patients (82.5%) in the DAPHNe trial.
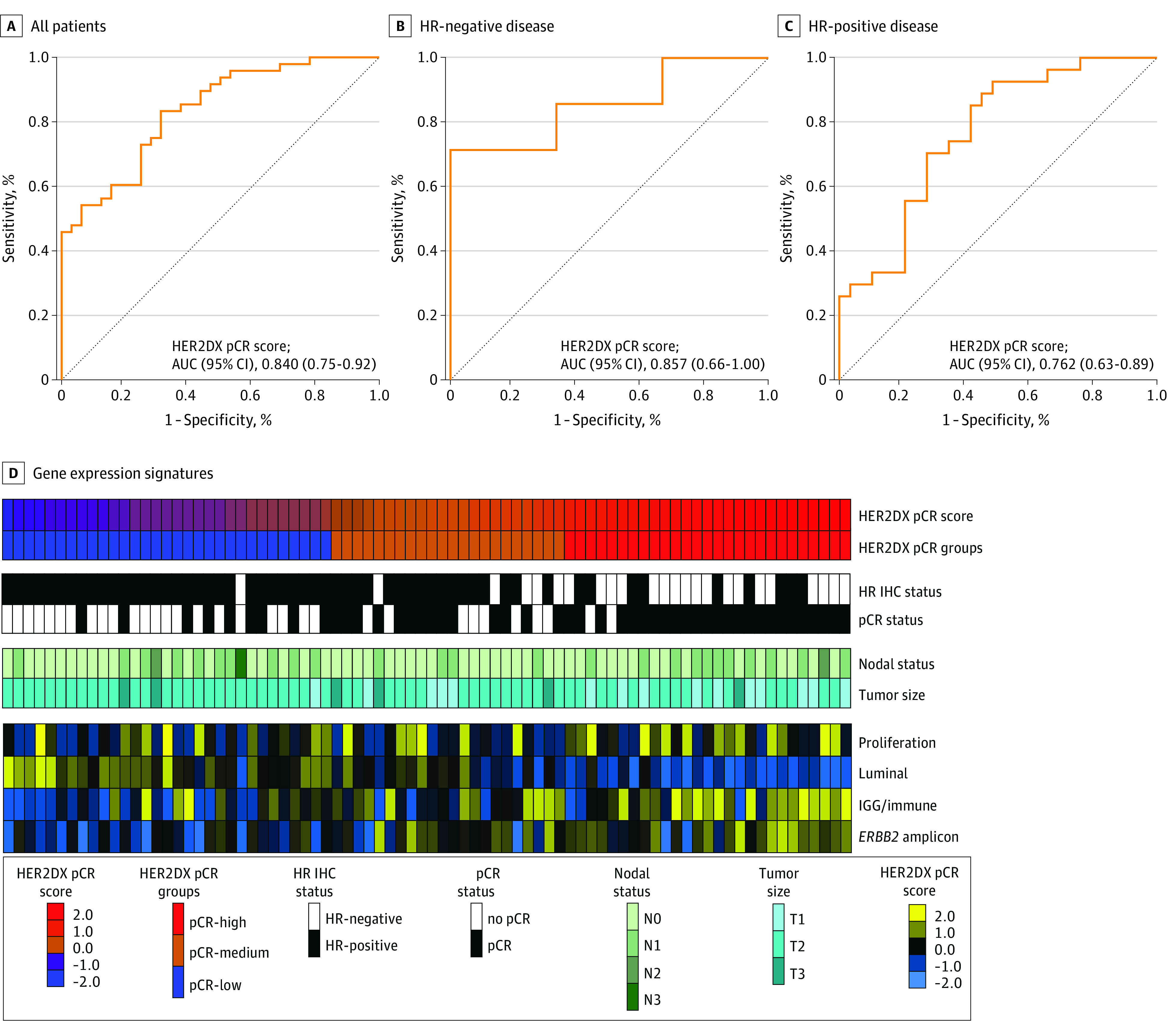
Main outcomes and measures: The primary aim was to test the ability of the HER2DX pCR likelihood score (as a continuous variable from 0-100) to predict pCR (ypT0/isN0).
Results: Of 80 participants, 79 (98.8%) were women and there were 4 African American (5.0%), 6 Asian (7.5%), 4 Hispanic (5.0%), and 66 White individuals (82.5%); the mean (range) age was 50.3 (26.0-78.0) years. The HER2DX pCR score was significantly associated with pCR (odds ratio, 1.05; 95% CI, 1.03-1.08; P < .001). The pCR rates in the HER2DX high, medium, and low pCR score groups were 92.6%, 63.6%, and 29.0%, respectively (high vs low odds ratio, 30.6; P < .001). The HER2DX pCR score was significantly associated with pCR independently of hormone receptor status, ERBB2 immunohistochemistry score, HER2DX ERBB2 expression score, and prediction analysis of microarray 50 ERBB2-enriched subtype. The correlation between the HER2DX pCR score and prognostic risk score was weak (Pearson coefficient, -0.12). Performance of the risk score could not be assessed due to lack of recurrence events.
Conclusions and relevance: The results of this diagnostic/prognostic study suggest that the HER2DX pCR score assay could predict pCR following treatment with deescalated neoadjuvant paclitaxel with trastuzumab and pertuzumab in patients with early-stage ERBB2+ BC. The HER2DX pCR score might guide therapeutic decisions by identifying patients who are candidates for deescalated or escalated approaches.
Conflict of interest statement
Figures
References
-
- Yau C, Osdoit M, van der Noordaa M, et al. ; I-SPY 2 Trial Consortium . Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol. 2022;23(1):149-160. doi:10.1016/S1470-2045(21)00589-1 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
