

Machine learning links unresolving secondary pneumonia to mortality in patients with severe pneumonia, including COVID-19
- PMID: 37104035
- PMCID: PMC10266785
- DOI: 10.1172/JCI170682
Machine learning links unresolving secondary pneumonia to mortality in patients with severe pneumonia, including COVID-19
Abstract
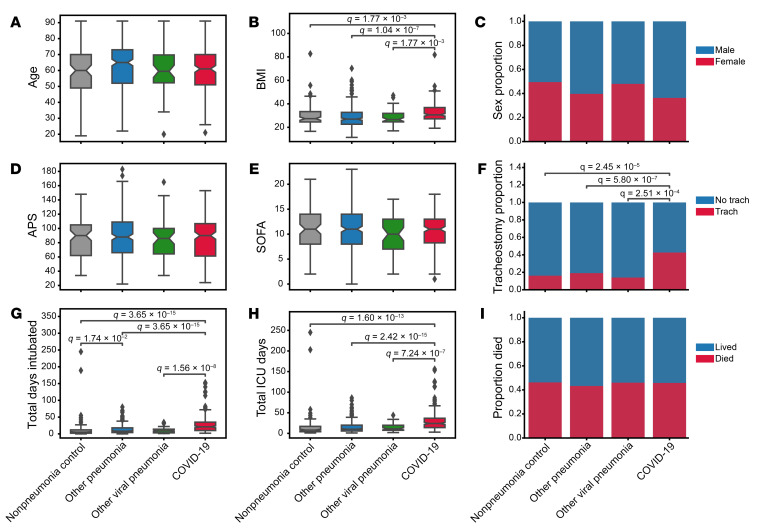
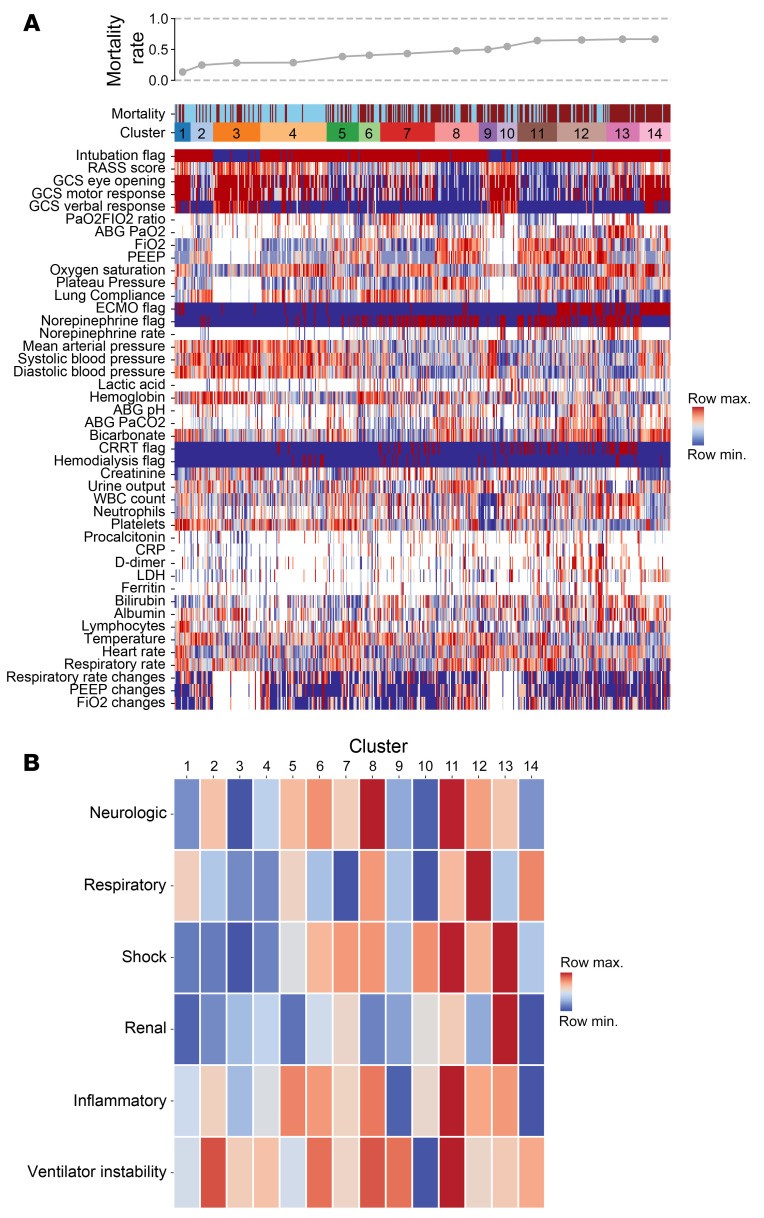
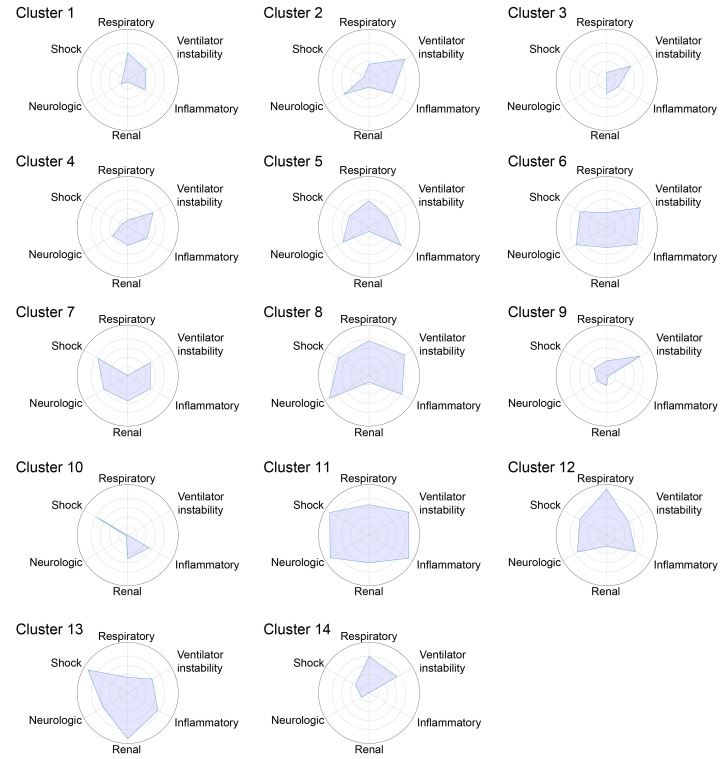
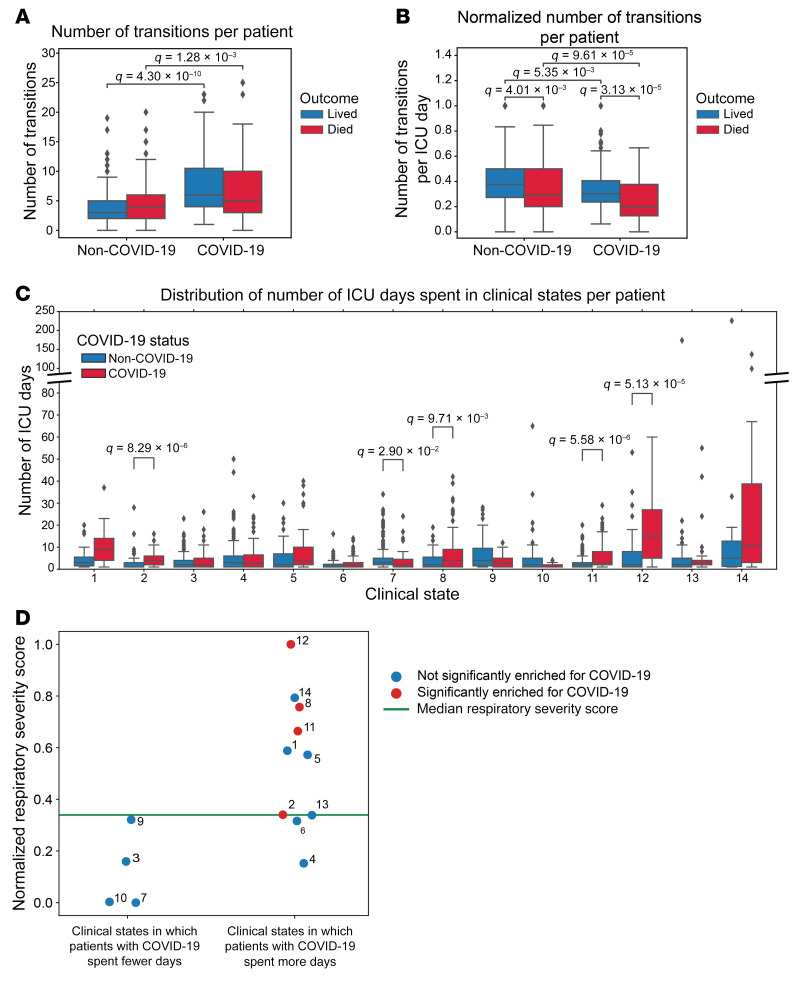
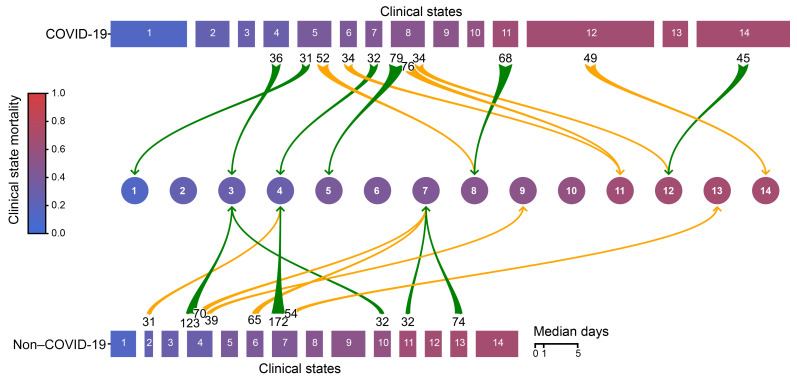
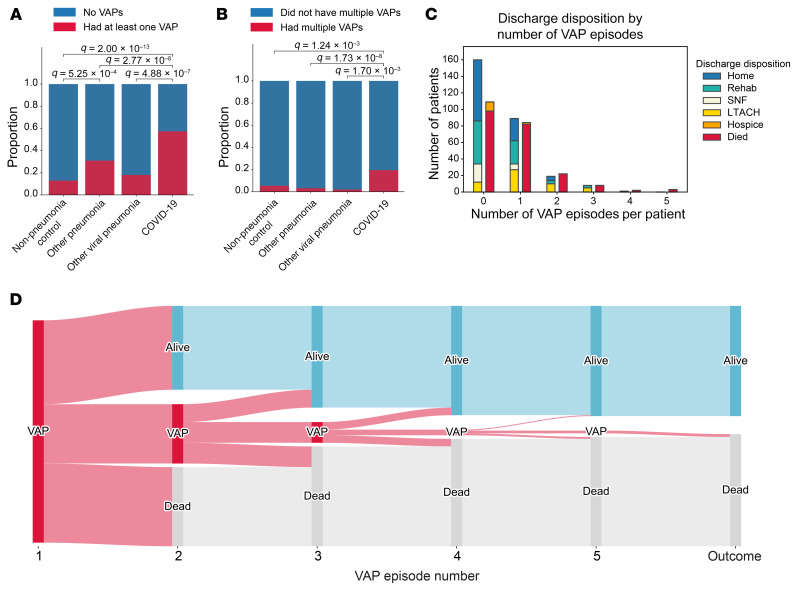
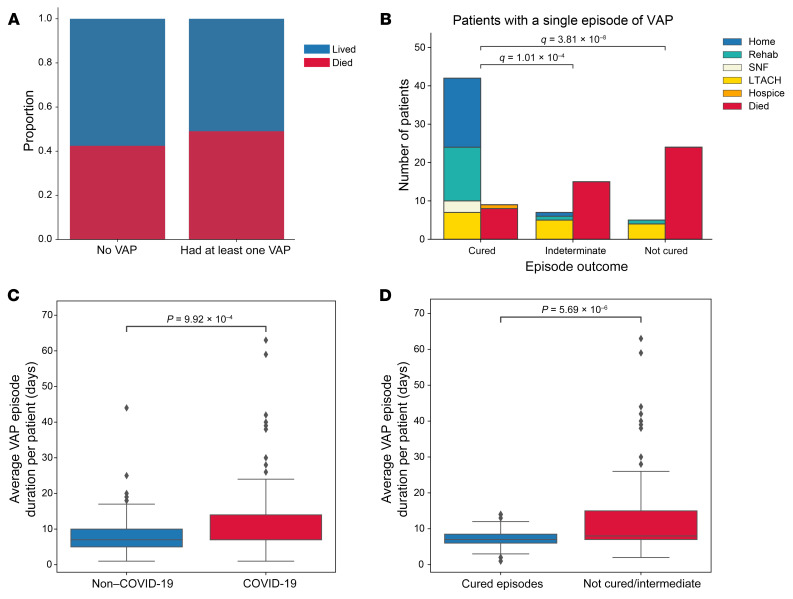
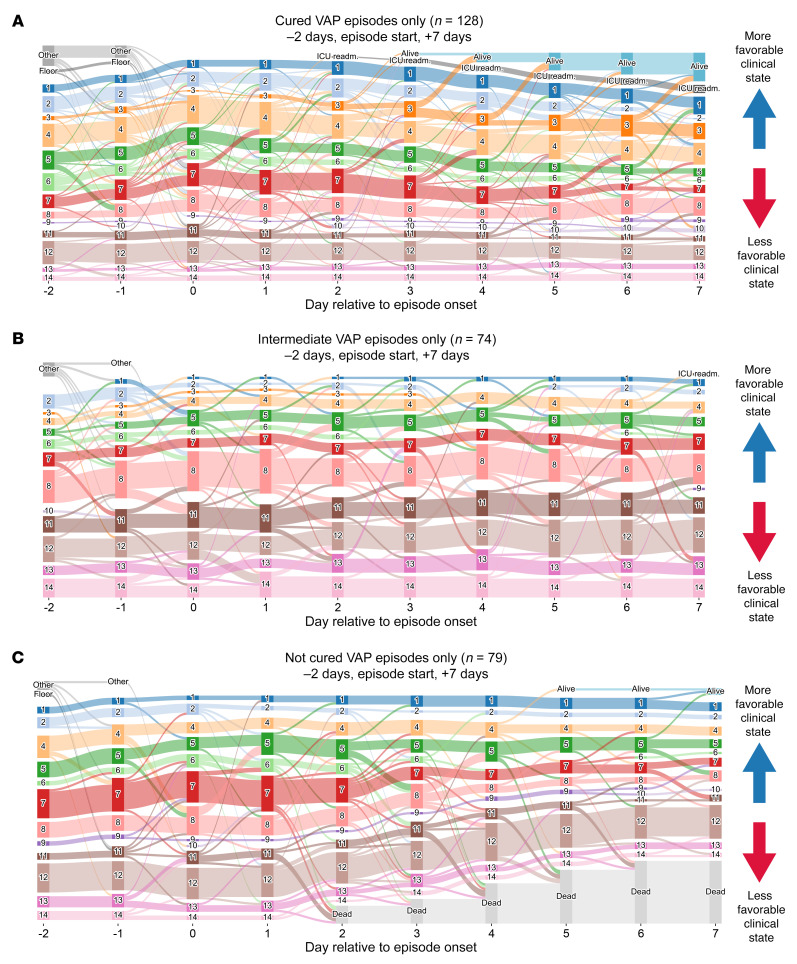
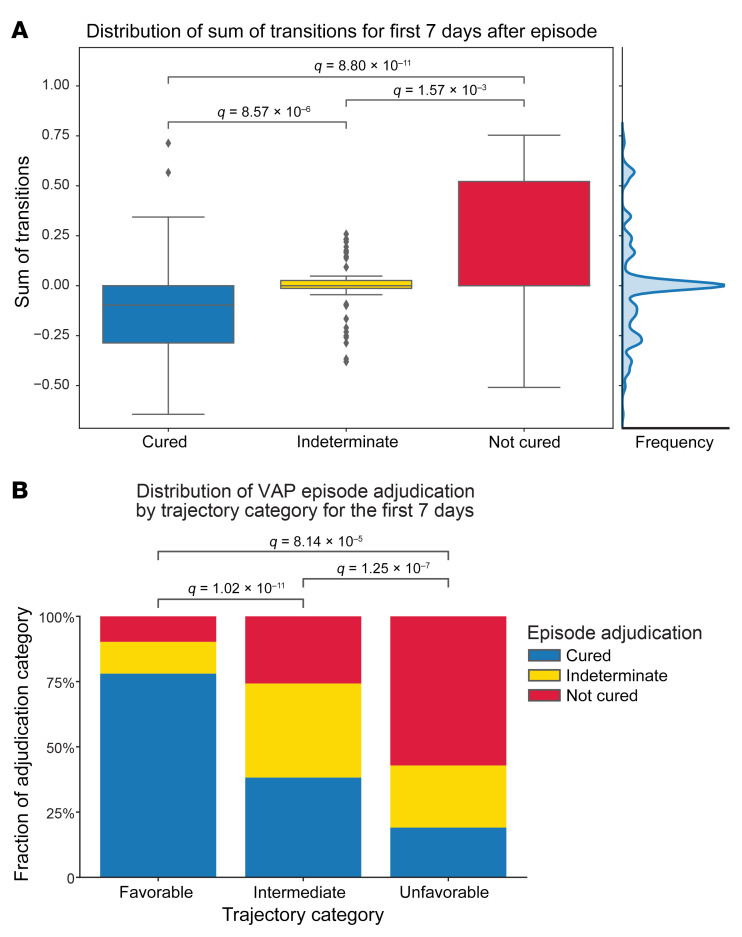
BACKGROUNDDespite guidelines promoting the prevention and aggressive treatment of ventilator-associated pneumonia (VAP), the importance of VAP as a driver of outcomes in mechanically ventilated patients, including patients with severe COVID-19, remains unclear. We aimed to determine the contribution of unsuccessful treatment of VAP to mortality for patients with severe pneumonia.METHODSWe performed a single-center, prospective cohort study of 585 mechanically ventilated patients with severe pneumonia and respiratory failure, 190 of whom had COVID-19, who underwent at least 1 bronchoalveolar lavage. A panel of intensive care unit (ICU) physicians adjudicated the pneumonia episodes and endpoints on the basis of clinical and microbiological data. Given the relatively long ICU length of stay (LOS) among patients with COVID-19, we developed a machine-learning approach called CarpeDiem, which grouped similar ICU patient-days into clinical states based on electronic health record data.RESULTSCarpeDiem revealed that the long ICU LOS among patients with COVID-19 was attributable to long stays in clinical states characterized primarily by respiratory failure. While VAP was not associated with mortality overall, the mortality rate was higher for patients with 1 episode of unsuccessfully treated VAP compared with those with successfully treated VAP (76.4% versus 17.6%, P < 0.001). For all patients, including those with COVID-19, CarpeDiem demonstrated that unresolving VAP was associated with a transitions to clinical states associated with higher mortality.CONCLUSIONSUnsuccessful treatment of VAP is associated with higher mortality. The relatively long LOS for patients with COVID-19 was primarily due to prolonged respiratory failure, placing them at higher risk of VAP.FUNDINGNational Institute of Allergy and Infectious Diseases (NIAID), NIH grant U19AI135964; National Heart, Lung, and Blood Institute (NHLBI), NIH grants R01HL147575, R01HL149883, R01HL153122, R01HL153312, R01HL154686, R01HL158139, P01HL071643, and P01HL154998; National Heart, Lung, and Blood Institute (NHLBI), NIH training grants T32HL076139 and F32HL162377; National Institute on Aging (NIA), NIH grants K99AG068544, R21AG075423, and P01AG049665; National Library of Medicine (NLM), NIH grant R01LM013337; National Center for Advancing Translational Sciences (NCATS), NIH grant U01TR003528; Veterans Affairs grant I01CX001777; Chicago Biomedical Consortium grant; Northwestern University Dixon Translational Science Award; Simpson Querrey Lung Institute for Translational Science (SQLIFTS); Canning Thoracic Institute of Northwestern Medicine.
Keywords: Bacterial infections; Bioinformatics; Infectious disease; Pulmonology.
Figures
Comment in
-
Ventilator-associated pneumonia in ICU patients with severe pneumonia and respiratory failure.J Clin Invest. 2023 Jun 15;133(12):e172643. doi: 10.1172/JCI172643. J Clin Invest. 2023. PMID: 37317965 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
- I01 CX001777/CX/CSRD VA/United States
- R01 HL153122/HL/NHLBI NIH HHS/United States
- F32 HL162377/HL/NHLBI NIH HHS/United States
- R21 AG075423/AG/NIA NIH HHS/United States
- P01 AG049665/AG/NIA NIH HHS/United States
- P01 HL071643/HL/NHLBI NIH HHS/United States
- U19 AI135964/AI/NIAID NIH HHS/United States
- R01 HL153312/HL/NHLBI NIH HHS/United States
- R01 HL158139/HL/NHLBI NIH HHS/United States
- U01 TR003528/TR/NCATS NIH HHS/United States
- R01 LM013337/LM/NLM NIH HHS/United States
- R01 HL154686/HL/NHLBI NIH HHS/United States
- R01 HL147575/HL/NHLBI NIH HHS/United States
- R01 HL149883/HL/NHLBI NIH HHS/United States
- T32 HL076139/HL/NHLBI NIH HHS/United States
- K99 AG068544/AG/NIA NIH HHS/United States
- P01 HL154998/HL/NHLBI NIH HHS/United States
