

A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity
- PMID: 37104194
- PMCID: PMC10145352
- DOI: 10.3390/toxins15040256
A Bayesian Network Meta-Analysis and Systematic Review of Guidance Techniques in Botulinum Toxin Injections and Their Hierarchy in the Treatment of Limb Spasticity
Abstract
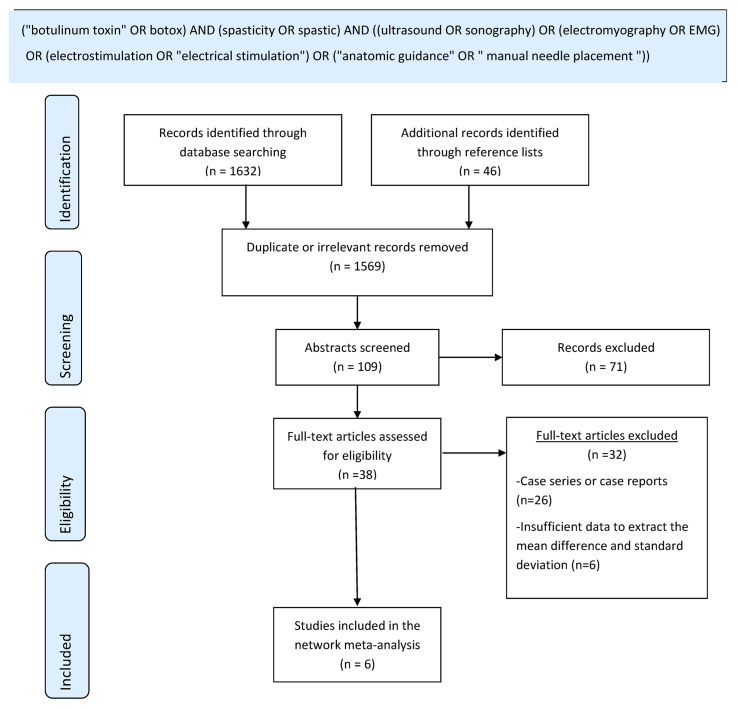
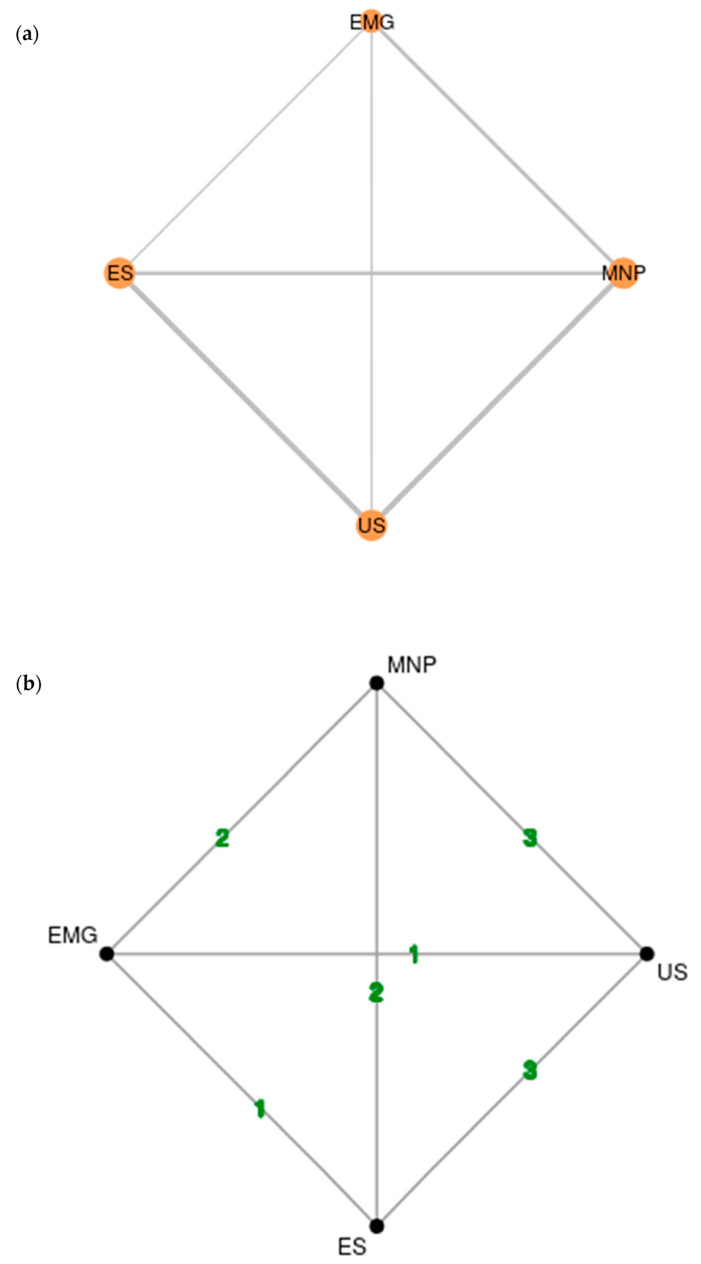
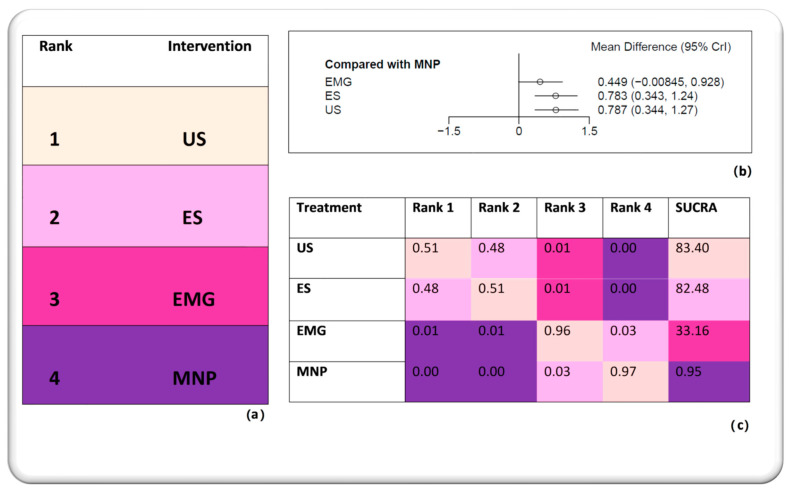
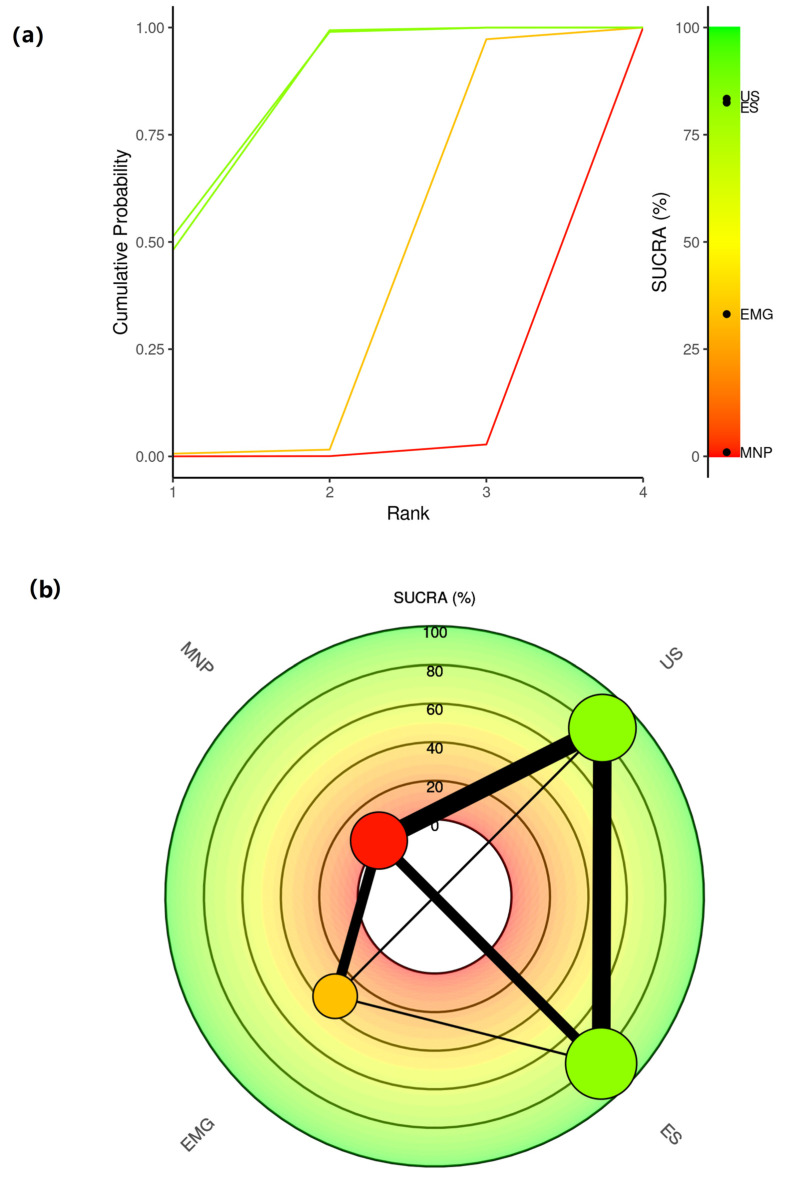
Accurate targeting of overactive muscles is fundamental for successful botulinum neurotoxin (BoNT) injections in the treatment of spasticity. The necessity of instrumented guidance and the superiority of one or more guidance techniques are ambiguous. Here, we sought to investigate if guided BoNT injections lead to a better clinical outcome in adults with limb spasticity compared to non-guided injections. We also aimed to elucidate the hierarchy of common guidance techniques including electromyography, electrostimulation, manual needle placement and ultrasound. To this end, we conducted a Bayesian network meta-analysis and systematic review with 245 patients using the MetaInsight software, R and the Cochrane Review Manager. Our study provided, for the first time, quantitative evidence supporting the superiority of guided BoNT injections over the non-guided ones. The hierarchy comprised ultrasound on the first level, electrostimulation on the second, electromyography on the third and manual needle placement on the last level. The difference between ultrasound and electrostimulation was minor and, thus, appropriate contextualization is essential for decision making. Taken together, guided BoNT injections based on ultrasound and electrostimulation performed by experienced practitioners lead to a better clinical outcome within the first month post-injection in adults with limb spasticity. In the present study, ultrasound performed slightly better, but large-scale trials should shed more light on which modality is superior.
Keywords: anatomical localization; botulinum neurotoxin; electromyography; electrostimulation; injections; limb spasticity; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Simpson D.M., Hallett M., Ashman E.J., Comella C.L., Green M.W., Gronseth G.S., Armstrong M.J., Gloss D., Potrebic S., Jankovic J., et al. Practice Guideline Update Summary: Botulinum Neurotoxin for the Treatment of Blepharospasm, Cervical Dystonia, Adult Spasticity, and Headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016;86:1818–1826. doi: 10.1212/WNL.0000000000002560. - DOI - PMC - PubMed
-
- Dressler D., Bhidayasiri R., Bohlega S., Chahidi A., Chung T.M., Ebke M., Jacinto L.J., Kaji R., Koçer S., Kanovsky P., et al. Botulinum Toxin Therapy for Treatment of Spasticity in Multiple Sclerosis: Review and Recommendations of the IAB Interdisciplinary Working Group for Movement Disorders Task Force. J. Neurol. 2017;264:112–120. doi: 10.1007/s00415-016-8304-z. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
