

A nutritional biomarker score of the Mediterranean diet and incident type 2 diabetes: Integrated analysis of data from the MedLey randomised controlled trial and the EPIC-InterAct case-cohort study
- PMID: 37104291
- PMCID: PMC10138823
- DOI: 10.1371/journal.pmed.1004221
A nutritional biomarker score of the Mediterranean diet and incident type 2 diabetes: Integrated analysis of data from the MedLey randomised controlled trial and the EPIC-InterAct case-cohort study
Abstract
Background: Self-reported adherence to the Mediterranean diet has been modestly inversely associated with incidence of type 2 diabetes (T2D) in cohort studies. There is uncertainty about the validity and magnitude of this association due to subjective reporting of diet. The association has not been evaluated using an objectively measured biomarker of the Mediterranean diet.
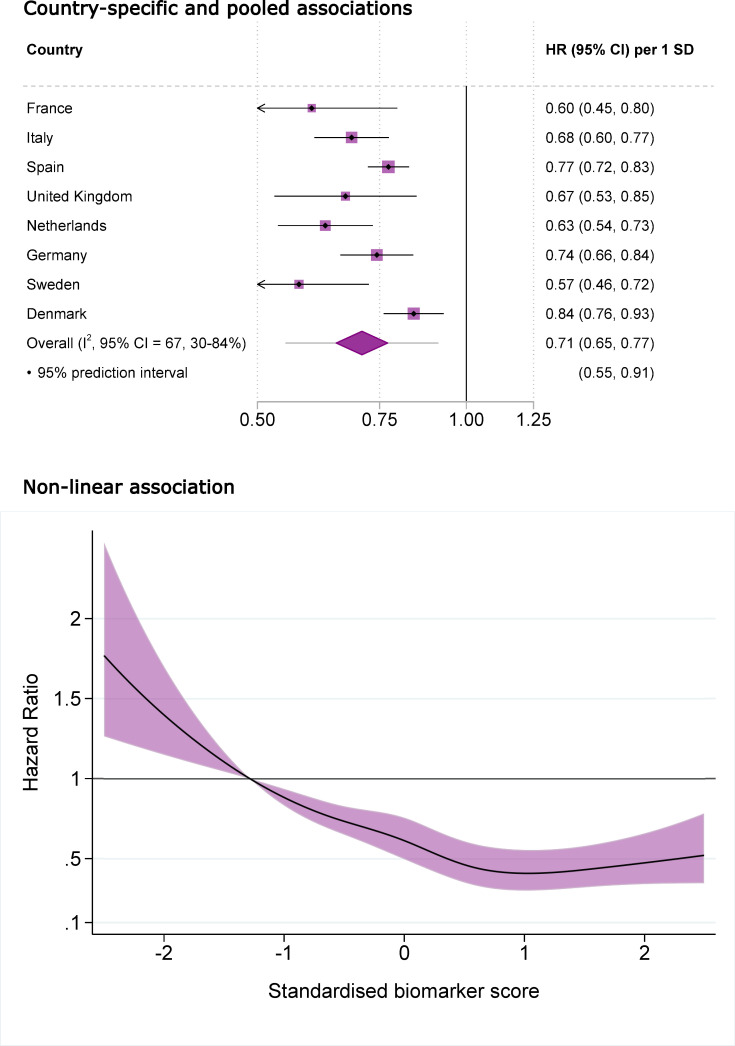
Methods and findings: We derived a biomarker score based on 5 circulating carotenoids and 24 fatty acids that discriminated between the Mediterranean or habitual diet arms of a parallel design, 6-month partial-feeding randomised controlled trial (RCT) conducted between 2013 and 2014, the MedLey trial (128 participants out of 166 randomised). We applied this biomarker score in an observational study, the European Prospective Investigation into Cancer and Nutrition (EPIC)-InterAct case-cohort study, to assess the association of the score with T2D incidence over an average of 9.7 years of follow-up since the baseline (1991 to 1998). We included 22,202 participants, of whom 9,453 were T2D cases, with relevant biomarkers from an original case-cohort of 27,779 participants sampled from a cohort of 340,234 people. As a secondary measure of the Mediterranean diet, we used a score estimated from dietary-self report. Within the trial, the biomarker score discriminated well between the 2 arms; the cross-validated C-statistic was 0.88 (95% confidence interval (CI) 0.82 to 0.94). The score was inversely associated with incident T2D in EPIC-InterAct: the hazard ratio (HR) per standard deviation of the score was 0.71 (95% CI: 0.65 to 0.77) following adjustment for sociodemographic, lifestyle and medical factors, and adiposity. In comparison, the HR per standard deviation of the self-reported Mediterranean diet was 0.90 (95% CI: 0.86 to 0.95). Assuming the score was causally associated with T2D, higher adherence to the Mediterranean diet in Western European adults by 10 percentiles of the score was estimated to reduce the incidence of T2D by 11% (95% CI: 7% to 14%). The study limitations included potential measurement error in nutritional biomarkers, unclear specificity of the biomarker score to the Mediterranean diet, and possible residual confounding.
Conclusions: These findings suggest that objectively assessed adherence to the Mediterranean diet is associated with lower risk of T2D and that even modestly higher adherence may have the potential to reduce the population burden of T2D meaningfully.
Trial registration: Australian New Zealand Clinical Trials Registry (ANZCTR) ACTRN12613000602729 https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=363860.
Copyright: © 2023 Sobiecki et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Authors declare support from the UK Medical Research Council, British Heart Foundation, Wellcome Trust, European Research Council, Swedish Research Council and National Institute for Health Research Cambridge Biomedical Research Centre for the submitted work. FI is a member of PLOS Medicine’s editorial board. PWF reports support for the submitted work from Novo Nordisk Foundation and consulting for Zoe Limited. JD reports grants, personal fees and non-financial support from Merck Sharp & Dohme (MSD), grants, personal fees and non-financial support from Novartis, grants from Pfizer and grants from AstraZeneca outside the submitted work. JD sits on the International Cardiovascular and Metabolic Advisory Board for Novartis (since 2010); the Steering Committee of UK Biobank (since 2011); the MRC International Advisory Group (ING) member, London (since 2013); the MRC High Throughput Science ‘Omics Panel Member, London (since 2013); the Scientific Advisory Committee for Sanofi (since 2013); the International Cardiovascular and Metabolism Research and Development Portfolio Committee for Novartis; and the Astra Zeneca Genomics Advisory Board (2018). ASB reports institutional grants outside the submitted work from AstraZeneca, Bayer, Biogen, BioMarin, Bioverativ, Novartis and Sanofi. Authors otherwise report no financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work.”
Figures

References
-
- Neuhouser ML, Pettinger M, Lampe JW, Tinker LF, George SM, Reedy J, et al.. Novel Application of Nutritional Biomarkers From a Controlled Feeding Study and an Observational Study to Characterization of Dietary Patterns in Postmenopausal Women. Am J Epidemiol. 2021;190:2461–2473. doi: 10.1093/aje/kwab171 - DOI - PMC - PubMed
