

Clinical progression, disease severity, and mortality among adults hospitalized with COVID-19 caused by the Omicron and Delta SARS-CoV-2 variants: A population-based, matched cohort study
- PMID: 37104488
- PMCID: PMC10138229
- DOI: 10.1371/journal.pone.0282806
Clinical progression, disease severity, and mortality among adults hospitalized with COVID-19 caused by the Omicron and Delta SARS-CoV-2 variants: A population-based, matched cohort study
Abstract
Background: To compare the intrinsic virulence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) omicron variant with the delta variant in hospitalized adults with coronavirus disease 2019 (COVID-19).
Methods: All adults hospitalized in the Capital Region of Copenhagen with a positive reverse transcription polymerase chain reaction test for SARS-CoV-2 and an available variant determination from 1 September 2021 to 11 February 2022. Data from health registries and patient files were used. Omicron and Delta patients were matched (1:1) by age, sex, comorbidities, and vaccination status. We calculated crude and adjusted hazard ratios (aHRs) for severe hypoxemia and mortality at 30 and 60 days.
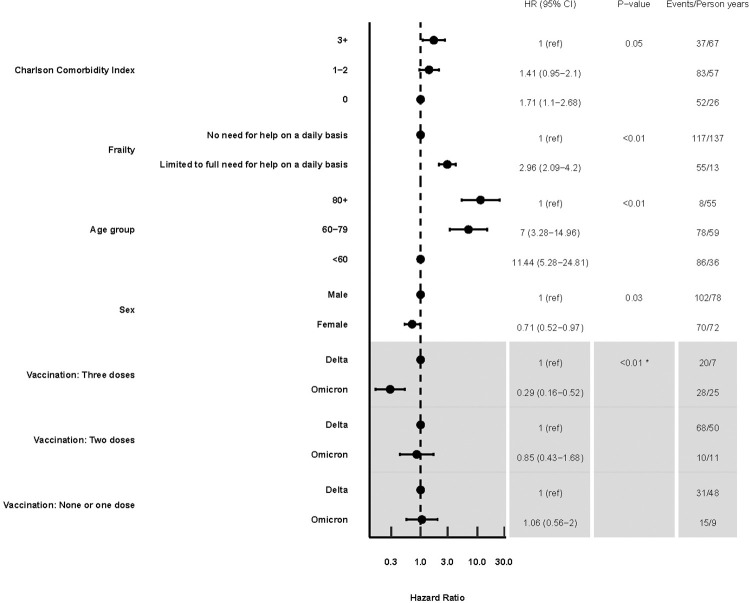
Results: 1,043 patients were included. Patients with Omicron were older, had more comorbidities, were frailer, and more often had three vaccine doses than those with Delta. Fewer patients with Omicron developed severe hypoxemia than those with Delta (aHR, 0.55; 95% confidence interval, 0.38-0.78). Omicron patients exhibited decreased aHR for 30-day mortality compared to Delta (aHR, 0.61; 0.39-0.95). Omicron patients who had received three vaccine doses had lower mortality compared to Delta patients who received three doses (aHR, 0.31;0.16-0.59), but not among those who received two or 0-1 doses (aHR, 0.86; 0.41-1.84 and 0.94; 0.49-1.81 respectively). Similar findings were observed for mortality at 60 days. Similar outcomes were obtained in the analyses of 316 individually matched patients.
Conclusions: Among adults hospitalized with COVID-19, those with Omicron had less severe hypoxemia and nearly 40% higher 30- and 60-day survival, as compared with those with Delta, mainly driven by a larger proportion of Omicron patients vaccinated with three doses of an mRNA vaccine.
Copyright: © 2023 COVID-19 Omicron Delta study group. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the following authors of this manuscript have declared that no competing interests exist: JGH, CKJ, PB, TGK, FIK, ANAA, SLM, BLJ, BBB, CS, TLN, LVH, BLM, AB, ME, PHB, EMJP, GBE, AMD, AS, IHMM, NZJ, PTP, MPGJ, TIP, RE, HESSR, MB, US, HA, MRS, PS, SA, JUSJ, KB, KMJ, MJSK, TL, UVS, MGA, SR, NlD, PR, NR, DP, AK, SJ, LEK, CL, BBH, OK, SRO, STS, AP, NK, MSP, LS, MV, LEC, MS AC, JF, AF, JW, RL, MR, TL, CR and TKF. I have read the journal’s policy and the following authors of this manuscript have following competing interests: ZBH has received research grants from Independent Research Fund Denmark (grant nr. 0134-00257B) and Lundbeck Foundation (grant nr. R349-2020-835). MvW was partially supported by the Independent Research Fund Denmark (grant # 8020-00284), and Carlsberg Foundation, Semper Ardens Research Project (grant # CF20-0046). LN received travel grants from MSD, GSK and Gilead. TB has received grants from Novo Nordisk Foundation, Lundbeck Foundation, Simonsen Foundation, GSK, Pfizer, Gilead, Kai Hansen Foundation and Erik and Susanna Olesen’s Charitable Fund and personal fees from GSK, Pfizer, Boehringer Ingelheim, Gilead, MSD, Pentabase ApS, Becton Dickinson, Janssen and Astra Zeneca, all outside the submitted work.
Figures
References
-
- World Health Organization Classification of omicron (B.1.1.529): SARS-CoV-2 variant of concern. Nov 26, 2021. https://www.who.int/news/item/26-11-2021- classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (Accessed May 1, 2020).
-
- World Health Organization Coronavirus Disease Dashboard. Available at https://covid19.who.int/. Last accessed May 01, 2022.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
