

Association between primary graft function and 5-year outcomes of islet allogeneic transplantation in type 1 diabetes: a retrospective, multicentre, observational cohort study in 1210 patients from the Collaborative Islet Transplant Registry
- PMID: 37105208
- PMCID: PMC10388704
- DOI: 10.1016/S2213-8587(23)00082-7
Association between primary graft function and 5-year outcomes of islet allogeneic transplantation in type 1 diabetes: a retrospective, multicentre, observational cohort study in 1210 patients from the Collaborative Islet Transplant Registry
Abstract
Background: Allogeneic islet transplantation is a validated therapy in type 1 diabetes; however, there is decline of transplanted islet graft function over time and the mechanisms underlying this decline are unclear. We evaluated the distinct association between primary graft function (PGF) and 5-year islet transplantation outcomes.
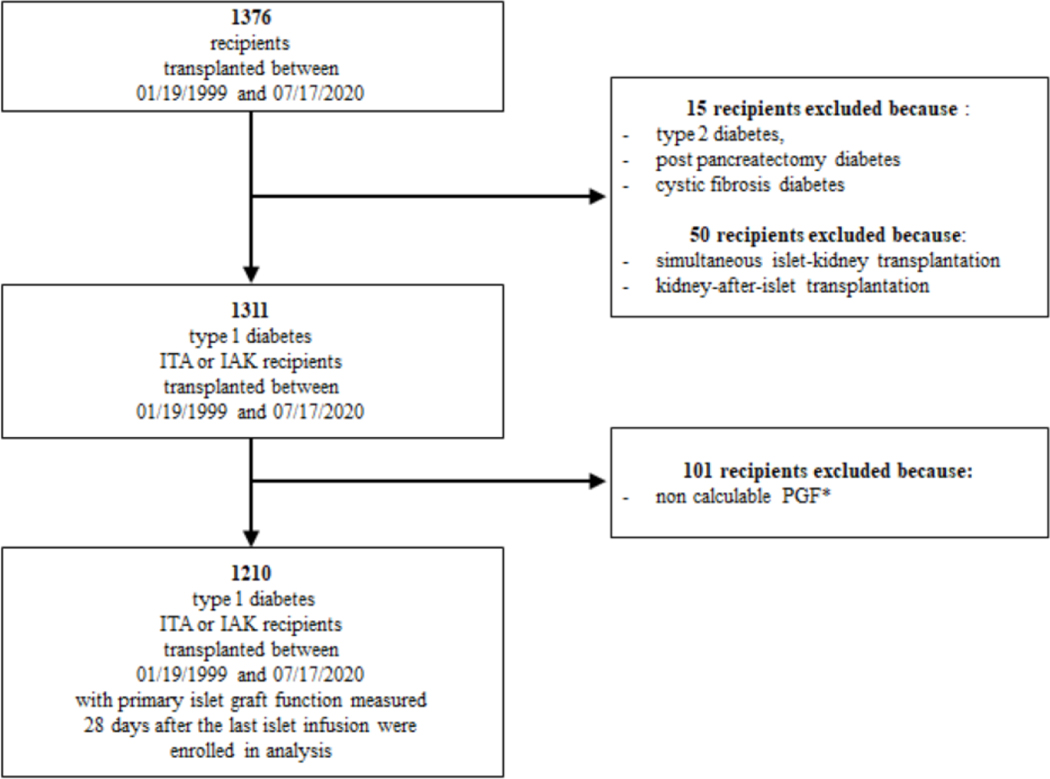
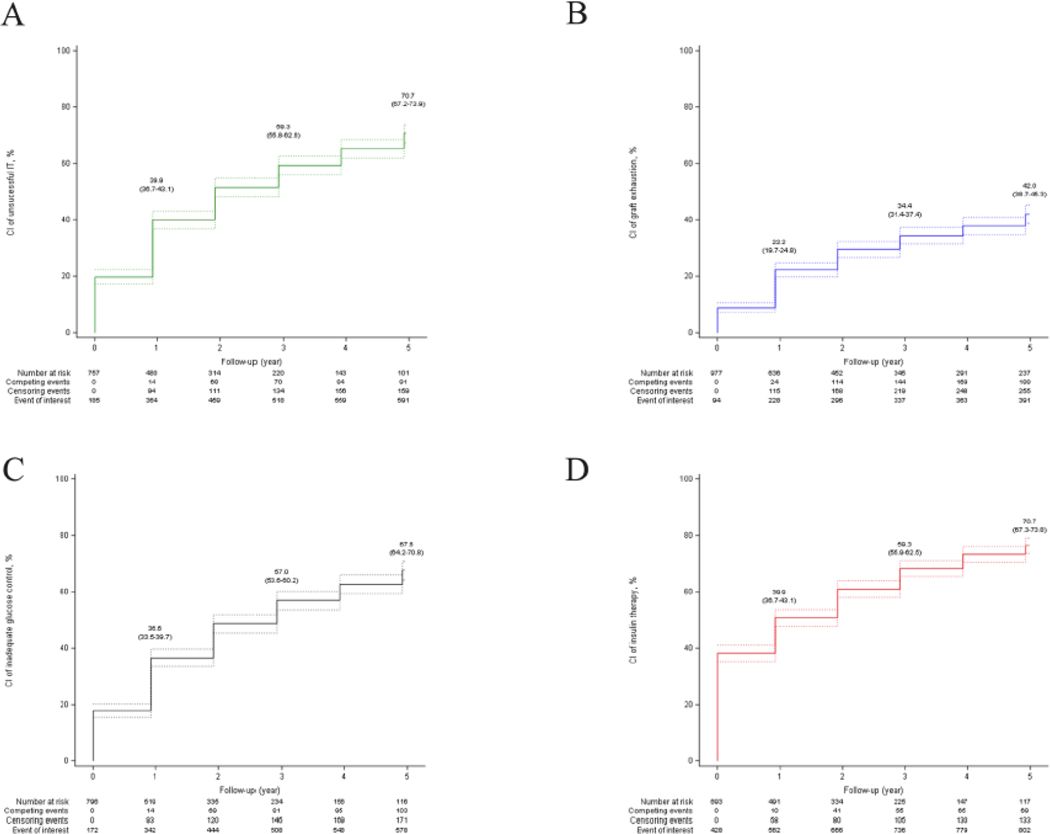
Methods: In this retrospective, multicentre, observational cohort study, we enrolled all patients from the Collaborative Islet Transplant Registry who received islet transplantation alone (ITA recipients) or islet-after-kidney transplantation (IAK recipients) between Jan 19, 1999, and July 17, 2020, with a calculable PGF (exposure of interest), measured 28 days after last islet infusion with a validated composite index of islet graft function (BETA-2 score). The primary outcome was cumulative incidence of unsuccessful islet transplantation, defined as an HbA1c of 7·0% (53 mmol/mol) or higher, or severe hypoglycaemia (ie, requiring third-party intervention to correct), or a fasting C-peptide concentration of less than 0·2 ng/mL. Secondary outcomes were graft exhaustion (fasting C-peptide <0·3 ng/mL); inadequate glucose control (HbA1c ≥7·0% [53 mmol/mol] or severe hypoglycaemia); and requirement for exogenous insulin therapy (≥14 consecutive days). Associations between PGF and islet transplantation outcomes were explored with a competing risk analysis adjusted for all covariates suspected or known to affect outcomes. A predictive model based on PGF was built and internally validated by using bootstraps resampling method.
Findings: In 39 centres worldwide, we enrolled 1210 patients with a calculable PGF (of those without missing data, mean age 47 years [SD 10], 712 [59·5%] were female, and 865 (97·9%) were White), who received a median of 10·8 thousand islet-equivalents per kg of bodyweight (IQR 7·4-13·5). 986 (82·4%) were ITA recipients and 211 (17·6%) were IAK recipients. Of 1210 patients, 452 (37·4%) received a single islet infusion and 758 (62·6%) received multiple islet infusions. Mean PGF was 14·3 (SD 8·8). The 5-year cumulative incidence of unsuccessful islet transplantation was 70·7% (95% CI 67·2-73·9), and was inversely and linearly related to PGF, with an adjusted subhazard ratio (sHR) of 0·77 (95% CI 0·72-0·82) per 5-unit increase of BETA-2 score (p<0·0001). Secondary endpoints were similarly related to PGF. The model-adjusted median C-statistic values of PGF for predicting 5-year cumulative incidences of unsuccessful islet transplantation, graft exhaustion, inadequate glucose control, and exogenous insulin therapy were 0·70 (range 0·69-0·71), 0·76 (0·74-0·77), 0·65 (0·64-0·66), and 0·72 (0·71-0·73), respectively.
Interpretation: This global multicentre study reports a linear and independent association between PGF and 5-year clinical outcomes of islet transplantation. The main study limitations are its retrospective design and the absence of analysis of complications.
Funding: Public Health Service Research, National Institutes of Health, Juvenile Diabetes Research Foundation International, Agence National de la Recherche, Fondation de l'Avenir, and Fonds de Dotation Line Renaud-Loulou Gasté.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests CB, EP and FB were employed by The EMMES Company. All other authors declare no competing interests.
Figures


Comment in
-
BETA-2 score at 28 days after islet allogeneic transplantation in type 1 diabetes for predicting 5-year outcomes.Lancet Diabetes Endocrinol. 2023 Jun;11(6):376-377. doi: 10.1016/S2213-8587(23)00090-6. Epub 2023 Apr 24. Lancet Diabetes Endocrinol. 2023. PMID: 37105209 No abstract available.
References
-
- CITR. Scientific Summary of the Collaborative Islet Transplant Registry (CITR), 11th Allograft Report. 2022. https://citregistry.org/
-
- Lablanche S, Vantyghem M-C, Kessler L, et al. Islet transplantation versus insulin therapy in patients with type 1 diabetes with severe hypoglycaemia or poorly controlled glycaemia after kidney transplantation (TRIMECO): a multicentre, randomised controlled trial. The Lancet Diabetes & Endocrinology 2018; 6: 527–37. - PubMed
-
- Vantyghem M, Marcelli-tourvieille S, Fermon C, et al. Intraperitoneal Insulin Infusion Versus Islet Transplantation: Comparative Study in Patients with Type 1 Diabetes. Transplantation 2009; 87: 66–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
